Touma Zahi, Costenbader Karen H, Hoskin Ben, Atkinson Christian, Bell David, Pike James, Berry Pamela, Karyekar Chetan S
University of Toronto, Toronto, Canada.
Brigham and Women's Hospital, Boston, MA, USA.
BMC Rheumatol. 2024 Jun 5;8(1):22. doi: 10.1186/s41927-023-00355-6.
Limited real-world data exists on clinical outcomes in systemic lupus erythematosus (SLE) patients by SLE Disease Activity Index 2000 (SLEDAI-2 K), hereafter, SLEDAI. We aimed to examine the association between SLEDAI score and clinical, patient-reported and economic outcomes in patients with SLE.
Rheumatologists from the United States of America and Europe provided real-world demographic, clinical, and healthcare resource utilization (HCRU) data for SLE patients. Patients provided self-reported outcome data, capturing their general health status using the EuroQol 5-dimension 3-level questionnaire (EQ-5D-3 L), health-related quality of life using the Functional Assessment of Chronic Illness Therapy (FACIT) and work productivity using the Work Productivity and Activity Impairment questionnaire (WPAI). Low disease activity was defined as SLEDAI score ≤ 4 and ≤ 7.5 mg/day glucocorticoids; patients not meeting these criteria were considered to have "higher" active disease. Data were compared between patients with low and higher disease activity. Logistic regression estimated a propensity score for SLE based on demographic and clinical characteristics. Propensity score matched analyses compared HCRU, patient-reported outcomes, income loss and treatment satisfaction in patients with low disease activity versus higher active disease.
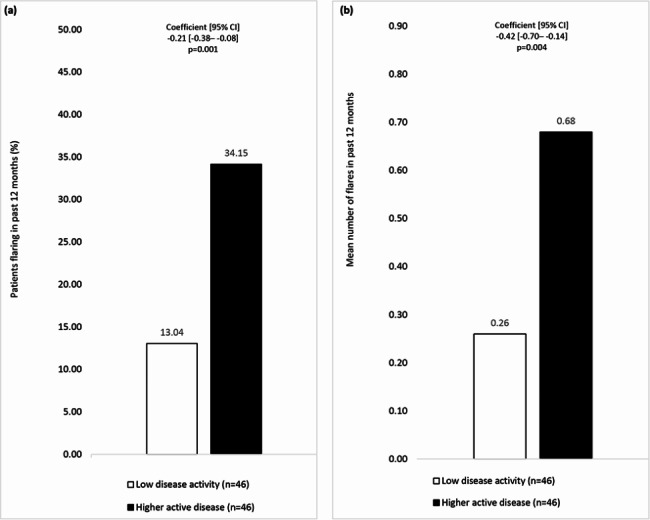
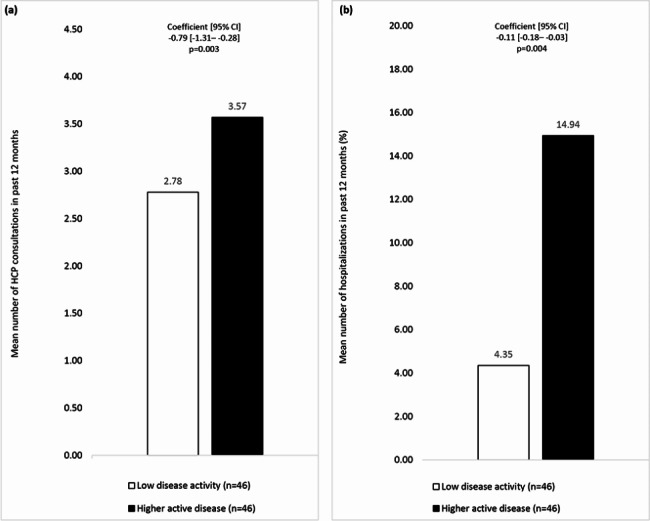
Data from 296 physicians reporting on 730 patients (46 low disease activity, 684 higher active disease), and from 377 patients' self-reported questionnaires (24 low disease activity, 353 higher active disease) were analyzed. Flaring in the previous 12 months was 2.6-fold more common among patients with higher versus low active disease. Equation 5D-3 L utility index was 0.79 and 0.88 and FACIT-Fatigue scores were 34.78 and 39.79 in low versus higher active disease patients, respectively, indicating better health and less fatigue, among patients with low versus higher active disease. Absenteeism, presenteeism, overall work impairment, and total activity impairment were 47.0-, 2.0-, 2.6- and 1.5-fold greater in patients with higher versus low disease activity. In the previous 12 months there were 28% more healthcare consultations and 3.4-fold more patients hospitalized in patients with higher versus low disease activity.
Compared to SLE patients with higher active disease, patients with low disease activity experienced better health status, lower HCRU, less fatigue, and lower work productivity impairment, with work absenteeism being substantially lower in these patients.
关于系统性红斑狼疮(SLE)患者使用2000年SLE疾病活动指数(SLEDAI - 2K,以下简称SLEDAI)的临床结局的真实世界数据有限。我们旨在研究SLE患者的SLEDAI评分与临床、患者报告结局及经济结局之间的关联。
来自美国和欧洲的风湿病学家提供了SLE患者的真实世界人口统计学、临床和医疗资源利用(HCRU)数据。患者提供自我报告的结局数据,使用欧洲五维健康量表(EQ - 5D - 3L)评估其总体健康状况,使用慢性病治疗功能评估量表(FACIT)评估健康相关生活质量,使用工作效率和活动障碍问卷(WPAI)评估工作效率。低疾病活动度定义为SLEDAI评分≤4且糖皮质激素用量≤7.5mg/天;未达到这些标准的患者被认为患有“更高”的活动性疾病。对低疾病活动度和高疾病活动度患者的数据进行比较。逻辑回归根据人口统计学和临床特征估计SLE的倾向评分。倾向评分匹配分析比较了低疾病活动度患者与高疾病活动度患者的HCRU、患者报告结局、收入损失和治疗满意度。
分析了来自296名医生报告的730例患者(46例低疾病活动度,684例高疾病活动度)的数据,以及来自377例患者自我报告问卷(24例低疾病活动度,353例高疾病活动度)的数据。在过去12个月中,高疾病活动度患者的病情复发比低疾病活动度患者常见2.6倍。低疾病活动度患者与高疾病活动度患者的EQ - 5D - 3L效用指数分别为0.79和0.88,FACIT - 疲劳评分分别为34.78和39.79,表明低疾病活动度患者的健康状况更好,疲劳程度更低。高疾病活动度患者的旷工、出勤但工作效率低下、总体工作障碍和总活动障碍分别是低疾病活动度患者的47.0倍、2.0倍、2.6倍和1.5倍。在过去12个月中,高疾病活动度患者的医疗咨询次数比低疾病活动度患者多28%,住院患者人数是低疾病活动度患者的3.4倍。
与高疾病活动度的SLE患者相比,低疾病活动度患者的健康状况更好,HCRU更低,疲劳程度更低,工作效率受损更低,这些患者的旷工率也显著更低。