Department of Cardiology, Heart Failure and Inherited Cardiac Diseases Unit, Hospital Universitario Puerta de Hierro Majadahonda, IDIPHISA, CIBERCV, Manuel de Falla, 2, Majadahonda, Madrid 28222, Spain.
Centro Nacional de Investigaciones Cardiovasculares Carlos III, Calle de Melchor Fernández Almagro, 3, Madrid, Spain.
Eur Heart J. 2024 Jul 9;45(26):2294-2305. doi: 10.1093/eurheartj/ehae362.
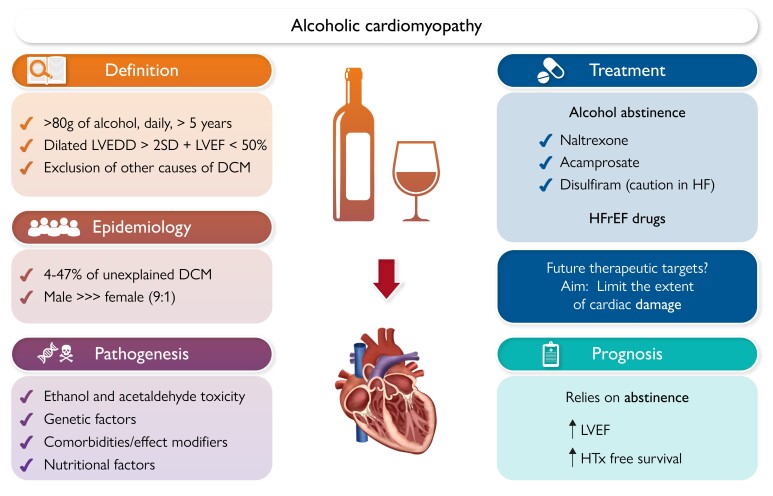
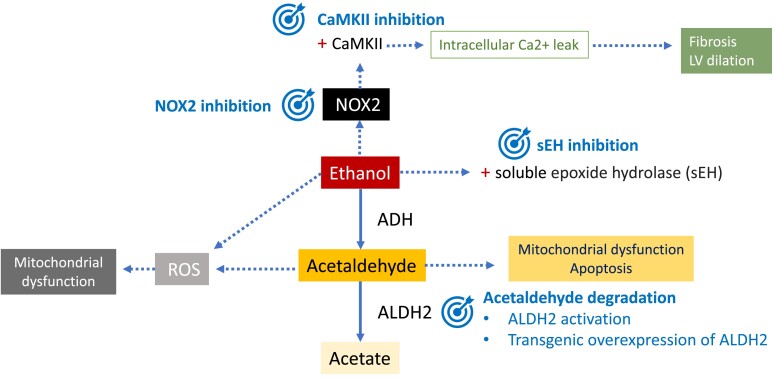
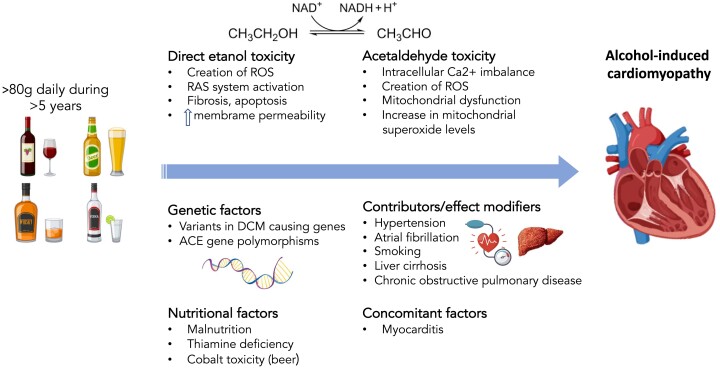
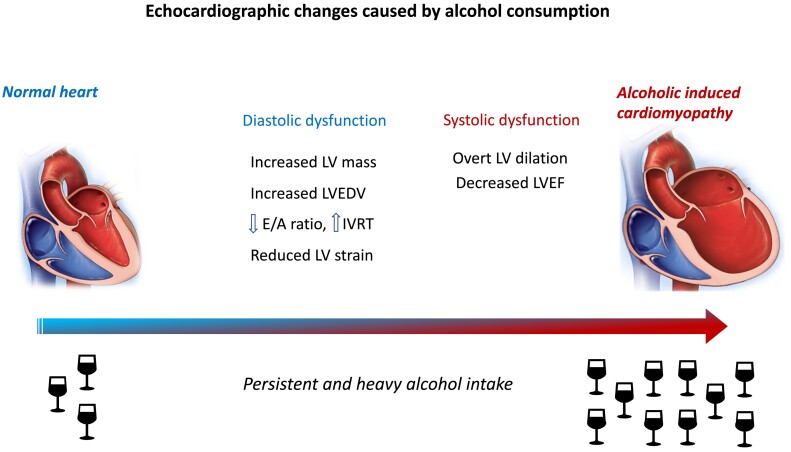
Alcohol-induced cardiomyopathy (AC) is an acquired form of dilated cardiomyopathy (DCM) caused by prolonged and heavy alcohol intake in the absence of other causes. The amount of alcohol required to produce AC is generally considered as >80 g/day over 5 years, but there is still some controversy regarding this definition. This review on AC focuses on pathogenesis, which involves different mechanisms. Firstly, the direct toxic effect of ethanol promotes oxidative stress in the myocardium and activation of the renin-angiotensin system. Moreover, acetaldehyde, the best-studied metabolite of alcohol, can contribute to myocardial damage impairing actin-myosin interaction and producing mitochondrial dysfunction. Genetic factors are also involved in the pathogenesis of AC, with DCM-causing genetic variants in patients with AC, especially titin-truncating variants. These findings support a double-hit hypothesis in AC, combining genetics and environmental factors. The synergistic effect of alcohol with concomitant conditions such as hypertension or liver cirrhosis can be another contributing factor leading to AC. There are no specific cardiac signs and symptoms in AC as compared with other forms of DCM. However, natural history of AC differs from DCM and relies directly on alcohol withdrawal, as left ventricular ejection fraction recovery in abstainers is associated with an excellent prognosis. Thus, abstinence from alcohol is the most crucial step in treating AC, and specific therapies are available for this purpose. Otherwise, AC should be treated according to current guidelines of heart failure with reduced ejection fraction. Targeted therapies based on AC pathogenesis are currently being developed and could potentially improve AC treatment in the future.
酒精性心肌病(AC)是一种获得性扩张型心肌病(DCM),由长期和大量饮酒引起,无其他原因。产生 AC 所需的酒精量通常被认为是 >80g/天,持续 5 年以上,但对于这个定义仍存在一些争议。这篇关于 AC 的综述主要关注发病机制,涉及不同的机制。首先,乙醇的直接毒性作用促进心肌中的氧化应激和肾素-血管紧张素系统的激活。此外,酒精的最佳研究代谢产物乙醛,可导致肌动球蛋白相互作用受损和线粒体功能障碍,从而导致心肌损伤。遗传因素也与 AC 的发病机制有关,AC 患者存在导致 DCM 的遗传变异,尤其是肌联蛋白截断变异。这些发现支持 AC 的双打击假说,即遗传因素和环境因素的协同作用。酒精与高血压或肝硬化等并存疾病的协同作用可能是导致 AC 的另一个因素。与其他类型的 DCM 相比,AC 没有特定的心脏体征和症状。然而,AC 的自然史与 DCM 不同,直接依赖于酒精戒断,因为戒酒者的左心室射血分数恢复与良好的预后相关。因此,戒酒是治疗 AC 的最关键步骤,为此目的提供了特定的治疗方法。否则,应根据射血分数降低的心力衰竭的现行指南治疗 AC。目前正在开发基于 AC 发病机制的靶向治疗方法,未来可能会改善 AC 的治疗效果。