Grummt Maximilian, Hafermann Lorena, Claussen Lars, Herrmann Carolin, Wolfarth Bernd
Department of Sports Medicine, Charité - Universitätsmedizin Berlin, Philippstr. 13 Haus 11, 10115, Berlin, Germany.
Institute of Biometry and Clinical Epidemiology, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität and Humboldt-Universität zu Berlin, Berlin, Germany.
Sports Med Open. 2024 Jun 10;10(1):71. doi: 10.1186/s40798-024-00729-1.
Physical inactivity is a growing risk factor worldwide, therefore getting people into sports is necessary. When prescribing physical activity, it is essential to recommend the correct training intensities. Cardiopulmonary exercise testing (CPX) enables precise determination of individuals' training intensities but is unavailable for a broad population. Therefore, the Borg scale allows individuals to assess perceived exertion and set their intensity easily and cost-efficiently. In order to transfer CPX to rating of perceived exertion (RPE), previous studies investigated RPE on specific physiological anchors, e.g. blood lactate (bLa) concentrations, but representativeness for a broad population is questionable. Some contradictory findings regarding individual factors influencing RPE occur, whereas univariable analysis has been performed so far. Moreover, a multivariable understanding of individual factors influencing RPE is missing. This study aims to determine RPE values at the individual anaerobic threshold (LT2) and defined bLa concentrations in a large cohort and to evaluate individual factors influencing RPE with multivariable analysis.
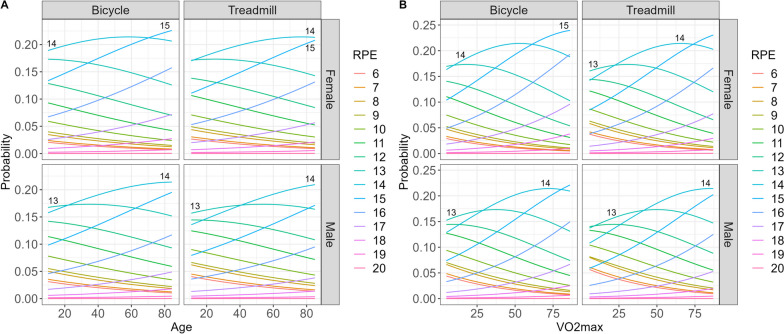
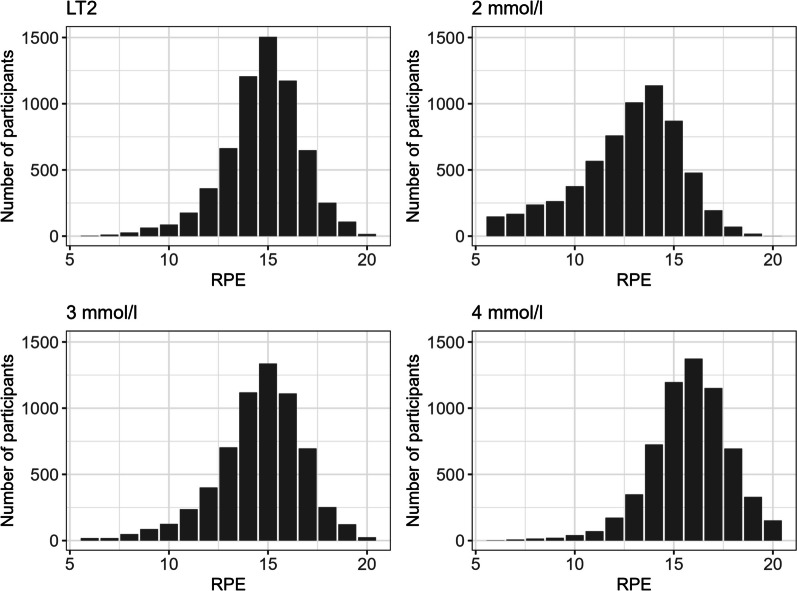
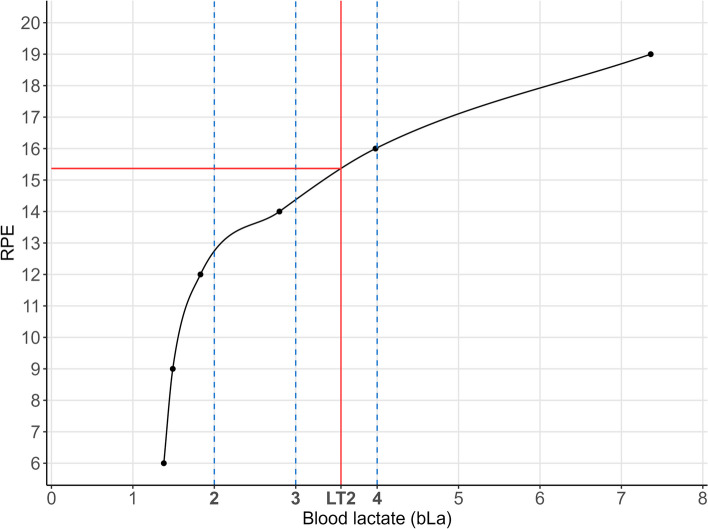
CPX with bicycle or treadmill ergometer of 6311 participants were analyzed in this cross-sectional study. RPE values at bLa concentrations 2 mmol/l, 3 mmol/l, 4 mmol/l, and LT2 (first rise in bLa over baseline + 1.5 mmol/l) were estimated by spline interpolation. Multivariable cumulative ordinal regression models were performed to assess the influence of sex, age, type of ergometry, VO2max, and duration of exercise testing on RPE.
Median values [interquartile range (IQR)] of the total population were RPE 13 [11; 14] at 2 mmol/l, RPE 15 [13; 16] at 3 mmol/l, RPE 16 [15; 17] at 4 mmol/l, and RPE 15 [14; 16] at LT2. Main influence of individual factors on RPE were seen especially at 2 mmol/l: male sex (odds ratio (OR) [95%-CI]: 0.65 [0.587; 0.719]), treadmill ergometry (OR 0.754 [0.641; 0.886]), number of stages (OR 1.345 [1.300; 1.394]), age (OR 1.015 [1.012; 1.018]), and VO2max (OR 1.023 [1.015; 1.030]). Number of stages was the only identified influencing factor on RPE at all lactate concentrations/LT2 (3 mmol/l: OR 1.290 [1.244; 1.336]; 4 mmol/l: OR 1.229 [1.187; 1.274]; LT2: OR 1.155 [1.115; 1.197]).
Our results suggest RPE ≤ 11 for light intensity, RPE 12-14 for moderate intensity, and RPE 15-17 for vigorous intensity, which slightly differs from the current American College of Sports Medicine (ACSM) recommendations. Additionally, we propose an RPE of 15 delineating heavy and severe intensity domain. Age, sex, type of ergometry, duration of exercise, and cardiopulmonary fitness should be considered when recommending individualized intensities with RPE, primarily at lower intensities. Therefore, this study can be used as a new guideline for prescribing individual RPE values in the clinical practice, predominantly for endurance type exercise.
缺乏身体活动在全球范围内正成为一个日益严重的风险因素,因此促使人们参与体育运动很有必要。在规定体育活动时,推荐正确的训练强度至关重要。心肺运动测试(CPX)能够精确测定个体的训练强度,但无法应用于广大人群。因此,伯格量表使个体能够轻松且经济高效地评估主观用力程度并设定自身强度。为了将CPX转换为自感用力度(RPE),以往研究针对特定生理指标(如血乳酸(bLa)浓度)研究了RPE,但对于广大人群的代表性存在疑问。关于影响RPE的个体因素出现了一些相互矛盾的研究结果,而且迄今为止仅进行了单变量分析。此外,尚缺乏对影响RPE的个体因素的多变量理解。本研究旨在确定一大群人在个体无氧阈(LT2)和特定bLa浓度下的RPE值,并通过多变量分析评估影响RPE的个体因素。
在这项横断面研究中,分析了6311名参与者使用自行车或跑步机测力计进行的CPX。通过样条插值法估算bLa浓度为2 mmol/l、3 mmol/l、4 mmol/l以及LT2(bLa超过基线的首次上升 + 1.5 mmol/l)时的RPE值。进行多变量累积有序回归模型以评估性别、年龄、测力计类型、最大摄氧量(VO2max)和运动测试持续时间对RPE的影响。
总体人群的中位数[四分位间距(IQR)]为,2 mmol/l时RPE为13[11;14],3 mmol/l时RPE为15[13;16],4 mmol/l时RPE为16[15;17],LT2时RPE为15[14;16]。个体因素对RPE的主要影响尤其在2 mmol/l时可见:男性(优势比(OR)[95%置信区间]:0.65[0.587;0.719])、跑步机测力计(OR 0.754[0.641;0.886])、阶段数(OR 1.345[1.300;1.394])、年龄(OR 1.015[1.012;1.018])和VO2max(OR 1.023[1.015;1.030])。阶段数是在所有乳酸浓度/LT2下唯一确定的影响RPE的因素(3 mmol/l:OR 1.290[1.244;1.336];4 mmol/l:OR 1.229[1.187;1.274];LT2:OR 1.155[1.115;1.197])。
我们的结果表明,轻度强度时RPE≤11,中度强度时RPE为12至14,剧烈强度时RPE为15至17,这与美国运动医学学院(ACSM)目前的建议略有不同。此外,我们提出RPE为15来划分重度和极重度强度范围。在通过RPE推荐个体化强度时,尤其是在较低强度时,应考虑年龄、性别、测力计类型、运动持续时间和心肺适能。因此,本研究可作为临床实践中开具个体RPE值的新指南,主要用于耐力型运动。