Institute of Infection and Immunity, St George's University and St Georges University Hospitals NHS Foundation Trust, London, United Kingdom.
Mycology Reference Centre Manchester and Department of Infectious Diseases, Manchester Academic Health Science Centre, Wythenshawe Hospital, Manchester University NHS Foundation Trust and Division of Evolution, Infection and Genomics, Faculty of Biology, Medicine and Health, University of Manchester, United Kingdom.
Clin Infect Dis. 2024 Jul 19;79(1):161-168. doi: 10.1093/cid/ciae239.
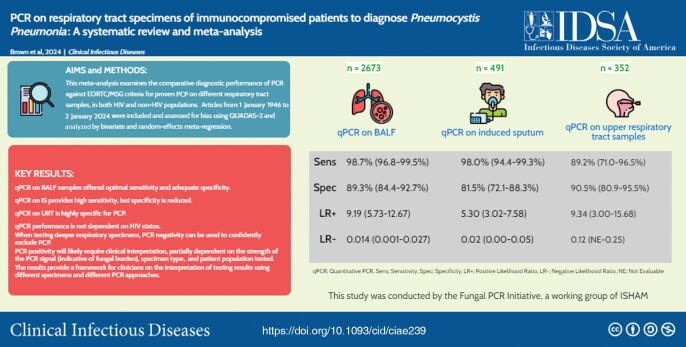
This meta-analysis examines the comparative diagnostic performance of polymerase chain reaction (PCR) for the diagnosis of Pneumocystis pneumonia (PCP) on different respiratory tract samples, in both human immunodeficiency virus (HIV) and non-HIV populations.
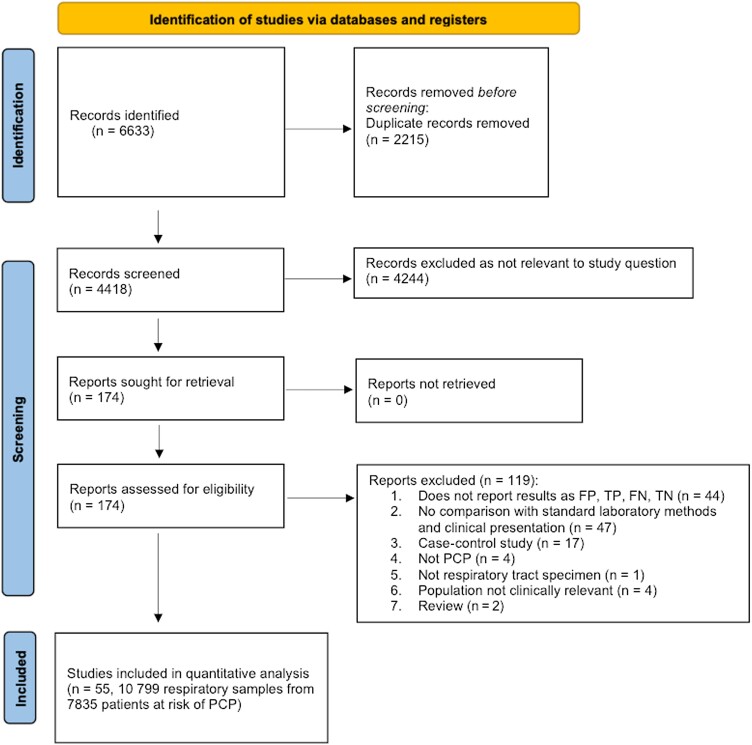
A total of 55 articles met inclusion criteria, including 11 434 PCR assays on respiratory specimens from 7835 patients at risk of PCP. QUADAS-2 tool indicated low risk of bias across all studies. Using a bivariate and random-effects meta-regression analysis, the diagnostic performance of PCR against the European Organisation for Research and Treatment of Cancer-Mycoses Study Group definition of proven PCP was examined.
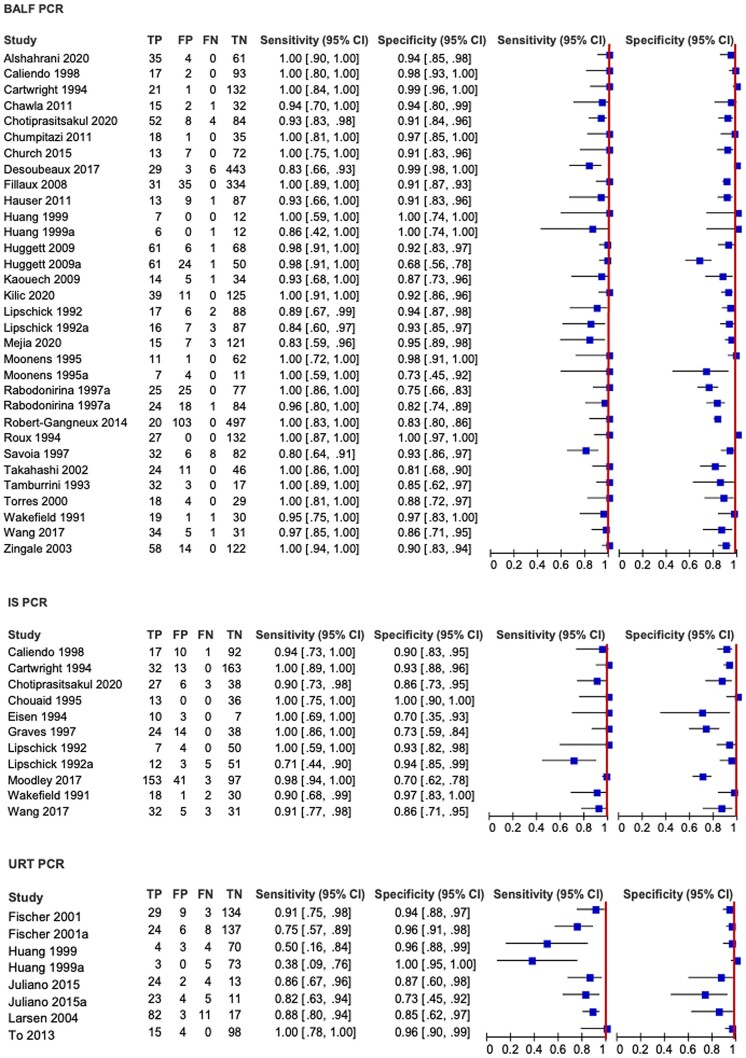
Quantitative PCR (qPCR) on bronchoalveolar lavage fluid provided the highest pooled sensitivity of 98.7% (95% confidence interval [CI], 96.8%-99.5%), adequate specificity of 89.3% (95% CI, 84.4%-92.7%), negative likelihood ratio (LR-) of 0.014, and positive likelihood ratio (LR+) of 9.19. qPCR on induced sputum provided similarly high sensitivity of 99.0% (95% CI, 94.4%-99.3%) but a reduced specificity of 81.5% (95% CI, 72.1%-88.3%), LR- of 0.024, and LR+ of 5.30. qPCR on upper respiratory tract samples provided lower sensitivity of 89.2% (95% CI, 71.0%-96.5%), high specificity of 90.5% (95% CI, 80.9%-95.5%), LR- of 0.120, and LR+ of 9.34. There was no significant difference in sensitivity and specificity of PCR according to HIV status of patients.
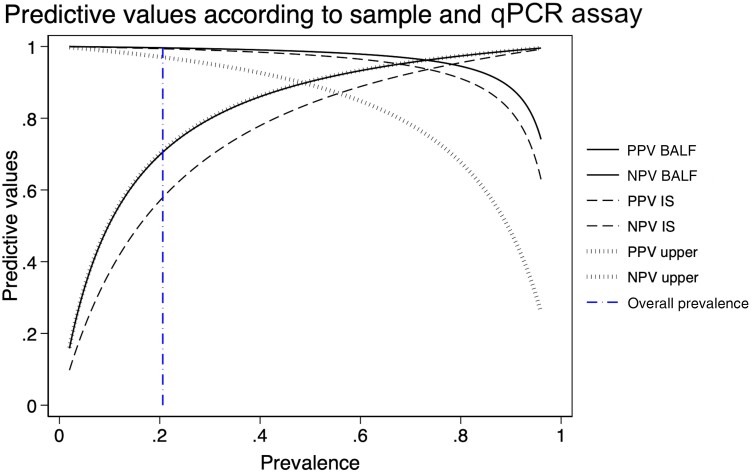
On deeper respiratory tract specimens, PCR negativity can be used to confidently exclude PCP, but PCR positivity will likely require clinical interpretation to distinguish between colonization and active infection, partially dependent on the strength of the PCR signal (indicative of fungal burden), the specimen type, and patient population tested.
本荟萃分析研究了聚合酶链反应(PCR)在不同呼吸道标本中对人类免疫缺陷病毒(HIV)和非 HIV 人群中肺孢子菌肺炎(PCP)的诊断比较诊断性能。
共有 55 篇文章符合纳入标准,包括 7835 名有 PCP 风险的患者的 11434 次呼吸道标本的 PCR 检测。QUADAS-2 工具表明所有研究的偏倚风险均较低。使用双变量和随机效应荟萃回归分析,检查了针对欧洲癌症研究与治疗组织-真菌病研究组确诊 PCP 定义的 PCR 诊断性能。
支气管肺泡灌洗液的定量 PCR(qPCR)提供了最高的合并敏感性 98.7%(95%置信区间 [CI],96.8%-99.5%),适当的特异性 89.3%(95%CI,84.4%-92.7%),阴性似然比(LR-)为 0.014,阳性似然比(LR+)为 9.19。诱导痰的 qPCR 提供了类似的高敏感性 99.0%(95%CI,94.4%-99.3%),但特异性降低至 81.5%(95%CI,72.1%-88.3%),LR-为 0.024,LR+为 5.30。上呼吸道标本的 qPCR 提供了较低的敏感性 89.2%(95%CI,71.0%-96.5%),高特异性 90.5%(95%CI,80.9%-95.5%),LR-为 0.120,LR+为 9.34。根据患者的 HIV 状态,PCR 的敏感性和特异性没有显著差异。
在更深的呼吸道标本中,PCR 阴性可用于有信心地排除 PCP,但 PCR 阳性可能需要临床解释来区分定植和感染,这部分取决于 PCR 信号的强度(提示真菌负荷)、标本类型和测试的患者人群。