Bloom Chloë I, Yang Freda, Hubbard Richard, Majeed Azeem, Wedzicha Jadwiga A
Imperial College London, National Heart and Lung Institute, London, United Kingdom of Great Britain and Northern Ireland;
Imperial College London, National Heart and Lung Institute, London, United Kingdom of Great Britain and Northern Ireland.
Am J Respir Crit Care Med. 2024 Aug 1;211(1):54-63. doi: 10.1164/rccm.202402-0368OC.
Inhaled corticosteroids (ICS) are the cornerstone of asthma treatment and significantly improve morbidity and mortality. Adverse effects of oral corticosteroids are well documented, but less is known about ICS.
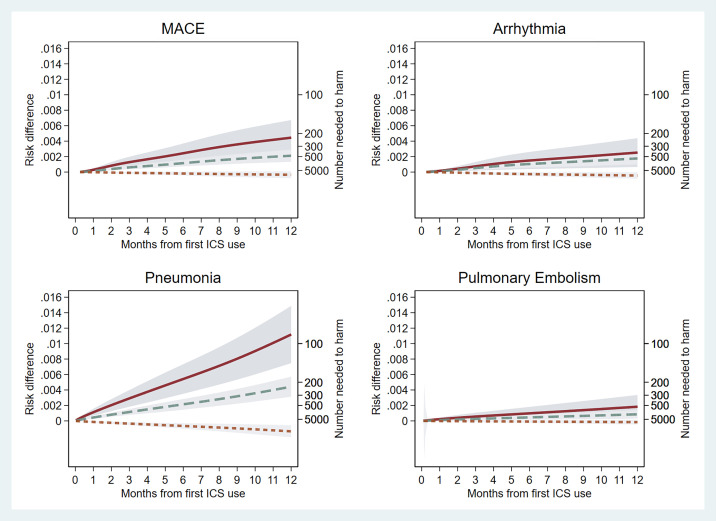
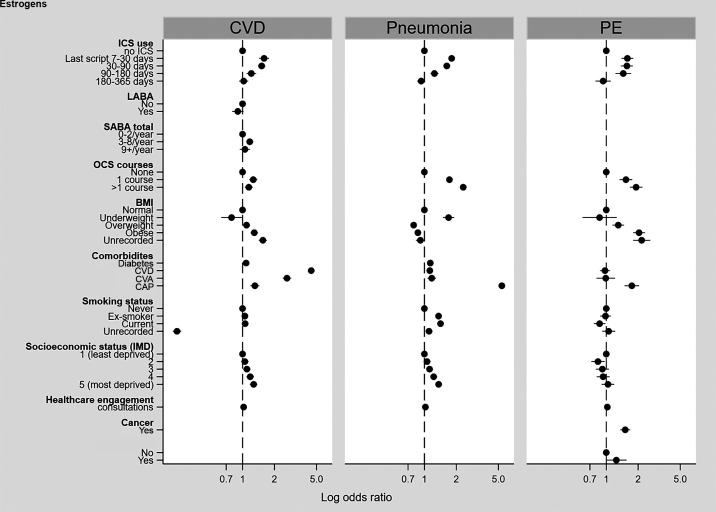
We conducted observational studies in adults with asthma using two different UK nationwide datasets: Clinical Practice Research Datalink (CPRD) Aurum and CPRD GOLD. The exposure was incident ICS; the outcomes were major adverse cardiac events (MACE), arrhythmia, pulmonary embolism (PE) and pneumonia over 12-months. Our main analyses used a cohort method with stabilized inverse probability treatment weighting to balance confounding between exposed and unexposed patients. Secondary analyses included nested case-control studies, and self-controlled case series. ICS was treated both as a categorical and continuous variable. Absolute risk was estimated using weighted flexible parametric models.
From 162,202 patients in our main cohort, there was an association with all outcomes at medium daily ICS dose or higher (HR, 95%CI at 201-599mcg: MACE=2.63, 1.66-4.15, arrhythmia=2.21, 1.60-3.04, PE=2.10, 1.37-3.22, pneumonia=2.25, 1.77-2.85; at ≥600mcg: MACE=4.63, 2.62-8.17, arrhythmia=2.91, 1.72-4.91, PE=3.32, 1.69-6.50, pneumonia=4.09, 2.98-5.60). There were no associations with lower doses of ICS. Secondary analyses produced similar results. The number needed to harm (95%CI) using 12-months of ICS 201-599mcg: MACE=473 (344-754), arrhythmia=567 (395-1006), PE=1221 (744-3388) and pneumonia=230 (177-327) and using ICS ≥600mcg: MACE=224 (148-461), arrhythmia=396 (228-1523), PE=577 (309-4311), pneumonia=93 (69-141).
Short-term use of low dose ICS was not associated with adverse effects. Moderate-high daily ICS doses were associated with an increased risk, but low-frequency, of cardiovascular events, pulmonary embolism and pneumonia. It is important for clinicians to adhere to guideline recommendations to use the lowest effective ICS dose. This article is open access and distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
吸入性糖皮质激素(ICS)是哮喘治疗的基石,可显著改善发病率和死亡率。口服糖皮质激素的不良反应已有充分记录,但关于ICS的了解较少。
我们使用英国两个不同的全国性数据集对成年哮喘患者进行了观察性研究:临床实践研究数据链(CPRD)金数据和CPRD奥鲁姆数据。暴露因素为新发ICS治疗;观察结局为12个月内的主要不良心脏事件(MACE)、心律失常、肺栓塞(PE)和肺炎。我们的主要分析采用队列法,并使用稳定的逆概率治疗权重来平衡暴露组和未暴露组患者之间的混杂因素。二次分析包括巢式病例对照研究和自我对照病例系列。ICS被视为分类变量和连续变量。使用加权灵活参数模型估计绝对风险。
在我们的主要队列中的162,202名患者中,中等每日ICS剂量及以上与所有结局均存在关联(HR,201 - 599mcg时的95%CI:MACE = 2.63,1.66 - 4.15;心律失常 = 2.21,1.60 - 3.04;PE = 2.10,1.37 - 3.22;肺炎 = 2.25,1.77 - 2.85;≥600mcg时:MACE = 4.63,2.62 - 8.17;心律失常 = 2.91,1.72 - 4.91;PE = 3.32,1.69 - 6.50;肺炎 = 4.09,2.98 - 5.60)。较低剂量的ICS未显示出关联。二次分析得出了类似的结果。使用12个月的201 - 599mcg ICS导致伤害的人数(95%CI):MACE = 473(344 - 754),心律失常 = 567(395 - 1006),PE = 1221(744 - 3388),肺炎 = 230(177 - 327);使用≥600mcg ICS时:MACE = 224(148 - 461),心律失常 = 39