Nielsen Mia-Louise, Petersen Troels C, Maul Lara Valeska, Thyssen Jacob P, Thomsen Simon F, Wu Jashin J, Navarini Alexander A, Kündig Thomas, Yawalkar Nikhil, Schlapbach Christoph, Boehncke Wolf-Henning, Conrad Curdin, Cozzio Antonio, Micheroli Raphael, Erik Kristensen Lars, Egeberg Alexander, Maul Julia-Tatjana
Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Copenhagen, Denmark.
Niels Bohr Institute, University of Copenhagen, Copenhagen, Denmark.
J Psoriasis Psoriatic Arthritis. 2024 Apr;9(2):41-50. doi: 10.1177/24755303231217492. Epub 2023 Nov 21.
Psoriatic arthritis (PsA) is a prevalent comorbidity among patients with psoriasis, heavily contributing to their burden of disease, usually diagnosed several years after the diagnosis of psoriasis.
To investigate the predictability of psoriatic arthritis in patients with psoriasis and to identify important predictors.
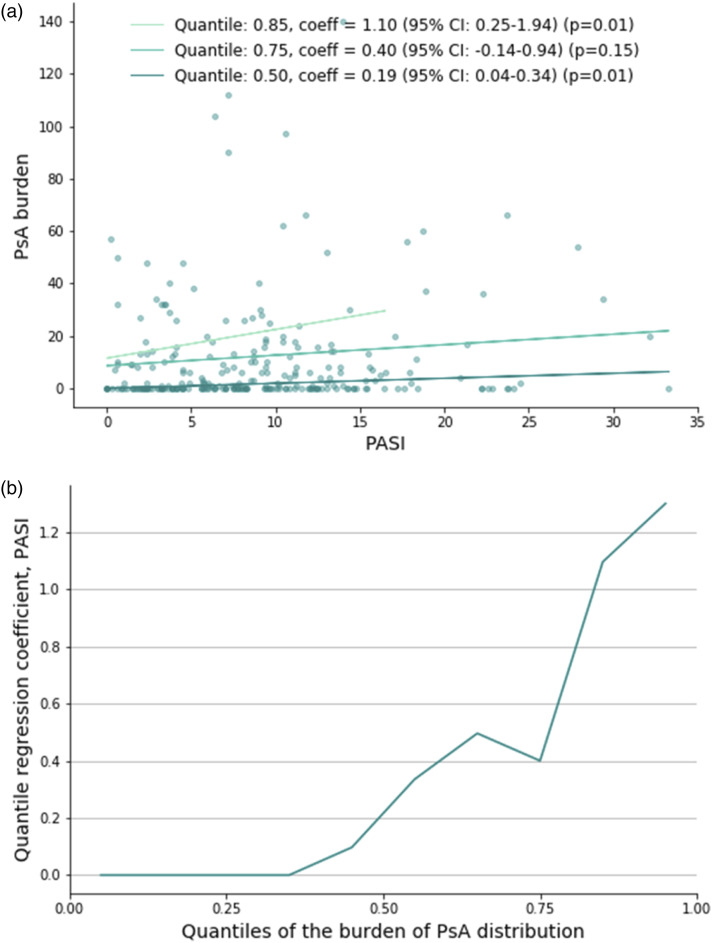
Data from the Swiss Dermatology Network on Targeted Therapies (SDNTT) involving patients treated for psoriasis were utilized. A combination of gradient-boosted decision trees and mixed models was used to classify patients based on their diagnosis of PsA or its absence. The variables with the highest predictive power were identified. Time to PsA diagnosis was visualized with the Kaplan-Meier method and the relationship between severity of psoriasis and PsA was explored through quantile regression.
A diagnosis of psoriatic arthritis was registered at baseline of 407 (29.5%) treatment series. 516 patients had no registration of PsA, 257 patients had PsA at inclusion, and 91 patients were diagnosed with PsA after inclusion. The model's AUROCs was up to 73.7%, and variables with the highest discriminatory power were age, PASI, physical well-being, and severity of nail psoriasis. Among patients who developed PsA after inclusion, significantly more first treatment series were classified in the PsA-group, compared to those with no PsA registration. PASI was significantly correlated with the median burden/severity of PsA ( = .01).
Distinguishing between patients with and without PsA based on clinical characteristics is feasible and even predicting future diagnoses of PsA is possible. Patients at higher risk can be identified using important predictors of PsA.
银屑病关节炎(PsA)是银屑病患者中常见的合并症,严重增加了他们的疾病负担,通常在银屑病诊断数年后才被诊断出来。
研究银屑病患者中银屑病关节炎的可预测性,并确定重要的预测因素。
利用瑞士皮肤病靶向治疗网络(SDNTT)中接受银屑病治疗患者的数据。采用梯度提升决策树和混合模型相结合的方法,根据患者是否诊断为PsA进行分类。确定预测能力最强的变量。采用Kaplan-Meier方法直观显示PsA诊断时间,并通过分位数回归探讨银屑病严重程度与PsA之间的关系。
在407个(29.5%)治疗系列的基线时记录到银屑病关节炎诊断。516例患者未记录有PsA,257例患者在纳入时患有PsA,91例患者在纳入后被诊断为PsA。该模型的曲线下面积(AUROC)高达73.7%,鉴别能力最强的变量是年龄、银屑病面积和严重程度指数(PASI)、身体健康状况和指甲银屑病严重程度。在纳入后发生PsA的患者中,与未记录有PsA的患者相比,更多的首次治疗系列被分类为PsA组。PASI与PsA的中位负担/严重程度显著相关(P = 0.01)。
根据临床特征区分有无PsA的患者是可行的,甚至预测PsA的未来诊断也是可能的。可以使用PsA的重要预测因素来识别高危患者。