Department of Population and Public Health Sciences (J.R.H., N.J.S., K.A., F.D.G., H.H., J.A.H., H.A.), Keck School of Medicine, University of Southern California, Los Angeles.
Department of Biochemistry and Molecular Medicine (J.R.H., N.J.S., K.A., H.A.), Keck School of Medicine, University of Southern California, Los Angeles.
Arterioscler Thromb Vasc Biol. 2024 Nov;44(11):2321-2333. doi: 10.1161/ATVBAHA.124.321001. Epub 2024 Oct 9.
COVID-19 is associated with acute risk of major adverse cardiac events (MACE), including myocardial infarction, stroke, and mortality (all-cause). However, the duration and underlying determinants of heightened risk of cardiovascular disease and MACE post-COVID-19 are not known.
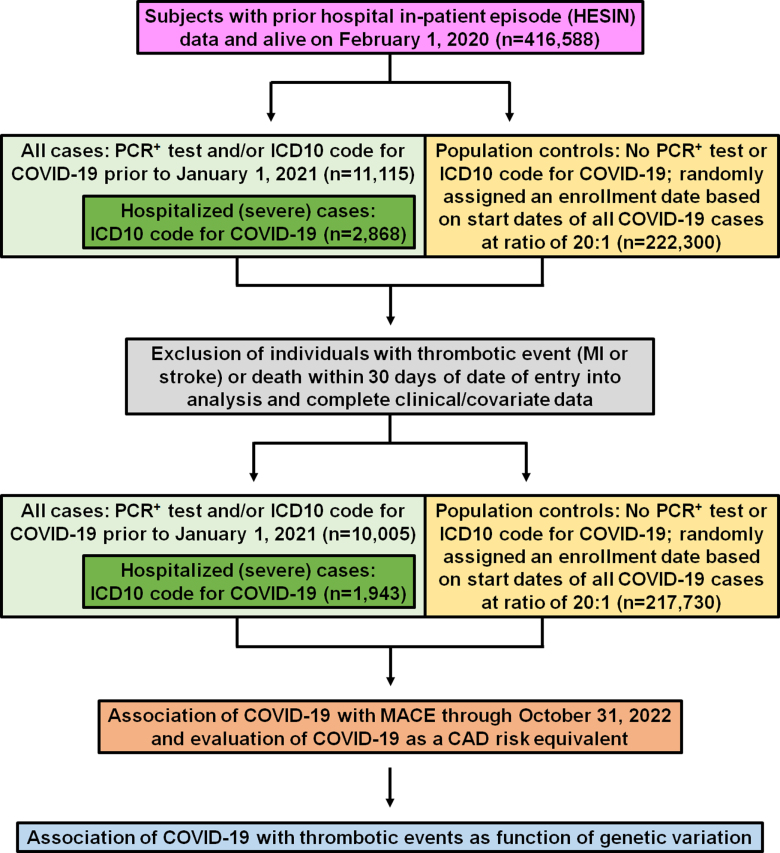
Data from the UK Biobank was used to identify COVID-19 cases (n=10 005) who were positive for polymerase chain reaction (PCR)-based tests for SARS-CoV-2 infection (n=8062) or received hospital-based ) codes for COVID-19 (n=1943) between February 1, 2020 and December 31, 2020. Population controls (n=217 730) and propensity score-matched controls (n=38 860) were also drawn from the UK Biobank during the same period. Proportional hazard models were used to evaluate COVID-19 for association with long-term (>1000 days) risk of MACE and as a coronary artery disease risk equivalent. Additional analyses examined whether COVID-19 interacted with genetic determinants to affect the risk of MACE and its components.
The risk of MACE was elevated in COVID-19 cases at all levels of severity (HR, 2.09 [95% CI, 1.94-2.25]; <0.0005) and to a greater extent in cases hospitalized for COVID-19 (HR, 3.85 [95% CI, 3.51-4.24]; <0.0005). Hospitalization for COVID-19 represented a coronary artery disease risk equivalent since incident MACE risk among cases without history of cardiovascular disease was even higher than that observed in patients with cardiovascular disease without COVID-19 (HR, 1.21 [95% CI, 1.08-1.37]; <0.005). A significant genetic interaction was observed between the locus and hospitalization for COVID-19 (=0.01), with risk of thrombotic events being increased in subjects with non-O blood types (HR, 1.65 [95% CI, 1.29-2.09]; =4.8×10) to a greater extent than subjects with blood type O (HR, 0.96 [95% CI, 0.66-1.39]; =0.82).
Hospitalization for COVID-19 represents a coronary artery disease risk equivalent, with post-acute myocardial infarction and stroke risk particularly heightened in non-O blood types. These results may have important clinical implications and represent, to our knowledge, one of the first examples of a gene-pathogen exposure interaction for thrombotic events.
COVID-19 与主要不良心脏事件(MACE)的急性风险相关,包括心肌梗死、中风和死亡率(全因)。然而,COVID-19 后心血管疾病和 MACE 风险增加的持续时间和潜在决定因素尚不清楚。
利用英国生物库的数据,确定了 2020 年 2 月 1 日至 12 月 31 日期间,聚合酶链反应(PCR)检测 SARS-CoV-2 感染呈阳性的 COVID-19 病例(n=10005)(n=8062)或因 COVID-19 住院的病例(n=1943)。同期还从英国生物库中抽取了人群对照(n=217730)和倾向评分匹配对照(n=38860)。使用比例风险模型评估 COVID-19 与长期(>1000 天)MACE 风险和冠心病风险相当的关联。其他分析还检查了 COVID-19 是否与遗传决定因素相互作用,从而影响 MACE 及其组成部分的风险。
在所有严重程度的 COVID-19 病例中,MACE 的风险均升高(HR,2.09[95%CI,1.94-2.25];<0.0005),因 COVID-19 住院的病例中风险升高更为明显(HR,3.85[95%CI,3.51-4.24];<0.0005)。COVID-19 住院治疗相当于冠心病风险,因为无心血管疾病史的病例发生 MACE 的风险甚至高于无 COVID-19 的心血管疾病患者(HR,1.21[95%CI,1.08-1.37];<0.005)。观察到 位点与 COVID-19 住院之间存在显著的遗传相互作用(=0.01),非 O 血型个体的血栓事件风险增加(HR,1.65[95%CI,1.29-2.09];=4.8×10)比 O 血型个体(HR,0.96[95%CI,0.66-1.39];=0.82)更明显。
COVID-19 住院治疗相当于冠心病风险,急性心肌梗死和中风风险在非 O 血型个体中尤其升高。这些结果可能具有重要的临床意义,代表了我们所知的第一个血栓事件的基因-病原体暴露相互作用的例子。