Švraka Dragan, Djurdjevic Svraka Anita, Djajic Vlado, Cucak Mile, Miskic Miso
Anesthesiology and Critical Care, Faculty of Medicine, University Clinical Center of Republic of Srpska/University of Banja Luka, Banja Luka, BIH.
Anesthesiology, Resuscitation, and Intensive Care, University Clinical Center of Republic of Srpska/General Hospital Gradiska, Gradiska, BIH.
Cureus. 2024 Sep 20;16(9):e69792. doi: 10.7759/cureus.69792. eCollection 2024 Sep.
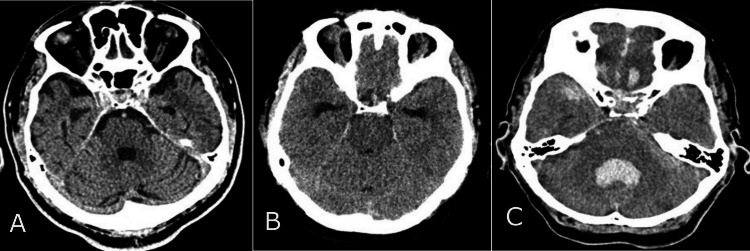
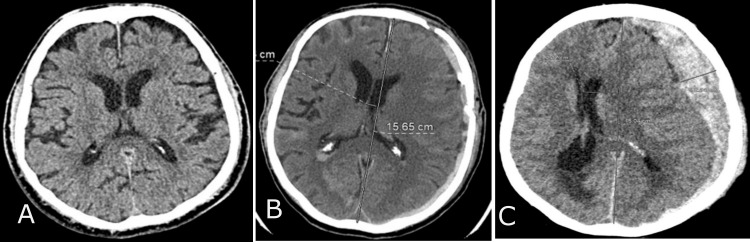
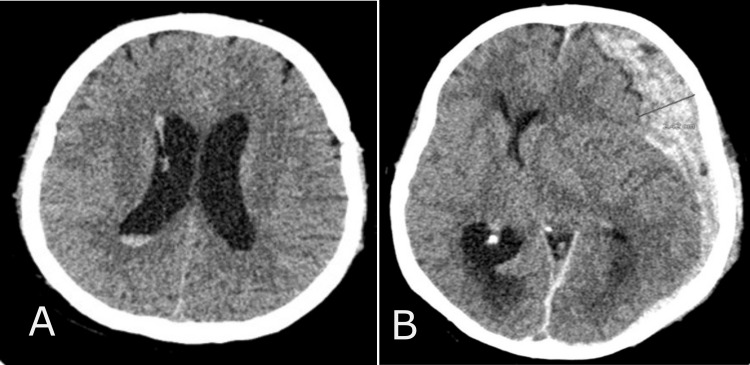
The Rotterdam scale is one of the most commonly used radiological scales for evaluating and predicting outcomes in traumatic brain injury (TBI) cases. Given the evolving nature of TBI, our study is designed to compare the Rotterdam score of computed tomography (CT) findings upon admission (Rotterdam score I) with the score after 72 hours (Rotterdam score II) of treatment in the trauma intensive care unit (ICU).
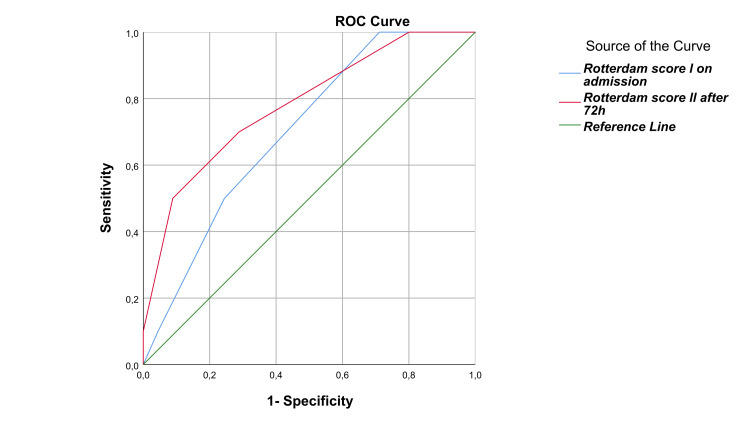
A retrospective observational study was conducted on 54 patients who received intensive care treatment for isolated severe TBI over five years. We included severe TBI patients with no age restrictions who required admission to the ICU within 12 hours of the onset of trauma. An initial Rotterdam CT score was obtained via a CT head scan within four hours of the trauma, followed by a control CT head scan 72 hours after ICU admission. It was essential to have documentation on the clinical and laboratory treatment course and access to radiological CT diagnostics. Receiver operating characteristic (ROC) curves were employed in this study to evaluate the accuracy of diagnostic tests, such as the Rotterdam score. The ROC curves provided a graphical representation of the tests' diagnostic performance, which helped assess their effectiveness.
There was a significant difference (p < 0.001) in the diagnostic scores of CT scans upon admission (Rotterdam score I) and control CT scans after 72 hours (Rotterdam score II) in the total sample. The Rotterdam score I was notably higher, 3.6 (±0.8), in patients requiring neurosurgical intervention compared to those who did not, 2.8 (±0.9), with significance (p = 0.003). The Rotterdam score I demonstrated a substantial predictive value for unfavorable outcomes (p = 0.048), as did the Rotterdam score II after the 72-hour mark (p = 0.006).
The control Rotterdam score 72 hours after admission predicts mortality in isolated TBI patients more significantly than the Rotterdam score determined at the patient's admission to the intensive care unit.
鹿特丹量表是评估和预测创伤性脑损伤(TBI)病例预后最常用的放射学量表之一。鉴于TBI的不断演变的性质,我们的研究旨在比较入院时计算机断层扫描(CT)结果的鹿特丹评分(鹿特丹评分I)与创伤重症监护病房(ICU)治疗72小时后的评分(鹿特丹评分II)。
对54例在五年内接受孤立性重度TBI重症监护治疗的患者进行了一项回顾性观察研究。我们纳入了无年龄限制的重度TBI患者,这些患者在创伤发生后12小时内需要入住ICU。在创伤后4小时内通过头颅CT扫描获得初始鹿特丹CT评分,随后在ICU入院72小时后进行对照头颅CT扫描。必须有临床和实验室治疗过程的记录以及放射学CT诊断结果。本研究采用受试者操作特征(ROC)曲线来评估诊断测试的准确性,如鹿特丹评分。ROC曲线提供了测试诊断性能的图形表示,有助于评估其有效性。
总样本中,入院时CT扫描的诊断评分(鹿特丹评分I)与72小时后的对照CT扫描(鹿特丹评分II)存在显著差异(p < 0.001)。与不需要神经外科干预的患者相比,需要神经外科干预的患者的鹿特丹评分I显著更高,分别为3.6(±0.8)和2.8(±0.9),具有显著性差异(p = 0.003)。鹿特丹评分I对不良预后具有显著的预测价值(p = 0.048),72小时后的鹿特丹评分II也是如此(p = 0.006)。
入院72小时后的对照鹿特丹评分比患者入住重症监护病房时确定的鹿特丹评分更能显著预测孤立性TBI患者的死亡率。