Department of Radiation Oncology, University of Utah, Salt Lake City, UT.
Artera, Inc, Los Altos, CA.
JCO Precis Oncol. 2024 Oct;8:e2400145. doi: 10.1200/PO.24.00145. Epub 2024 Oct 24.
Current clinical risk stratification methods for localized prostate cancer are suboptimal, leading to over- and undertreatment. Recently, machine learning approaches using digital histopathology have shown superior prognostic ability in phase III trials. This study aims to develop a clinically usable risk grouping system using multimodal artificial intelligence (MMAI) models that outperform current National Comprehensive Cancer Network (NCCN) risk groups.
The cohort comprised 9,787 patients with localized prostate cancer from eight NRG Oncology randomized phase III trials, treated with radiation therapy, androgen deprivation therapy, and/or chemotherapy. Locked MMAI models, which used digital histopathology images and clinical data, were applied to each patient. Expert consensus on cut points defined low-, intermediate-, and high-risk groups on the basis of 10-year distant metastasis rates of 3% and 10%, respectively. The MMAI's reclassification and prognostic performance were compared with the three-tier NCCN risk groups.
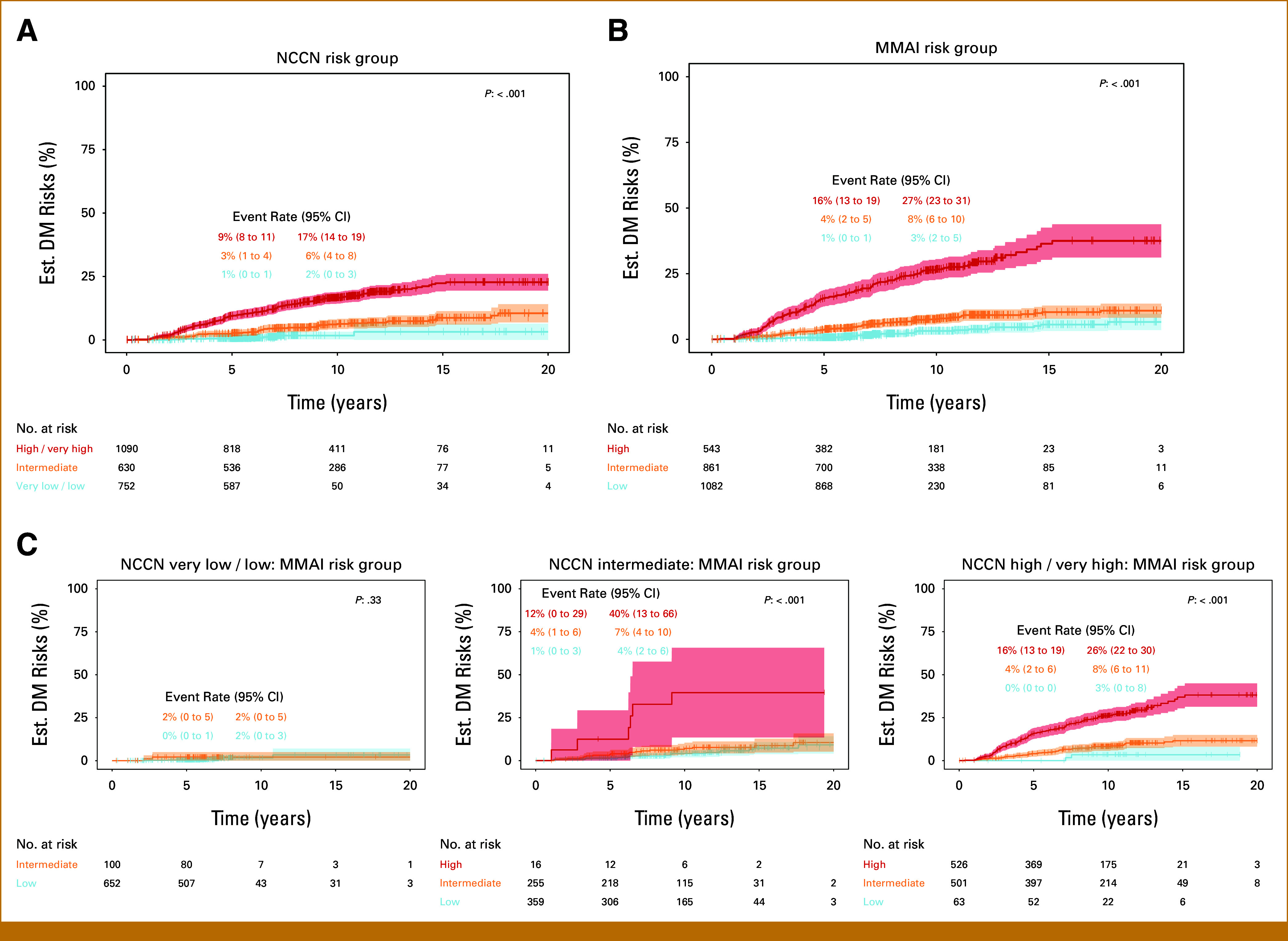
The median follow-up for censored patients was 7.9 years. According to NCCN risk categories, 30.4% of patients were low-risk, 25.5% intermediate-risk, and 44.1% high-risk. The MMAI risk classification identified 43.5% of patients as low-risk, 34.6% as intermediate-risk, and 21.8% as high-risk. MMAI reclassified 1,039 (42.0%) patients initially categorized by NCCN. Despite the MMAI low-risk group being larger than the NCCN low-risk group, the 10-year metastasis risks were comparable: 1.7% (95% CI, 0.2 to 3.2) for NCCN and 3.2% (95% CI, 1.7 to 4.7) for MMAI. The overall 10-year metastasis risk for NCCN high-risk patients was 16.6%, with MMAI further stratifying this group into low-, intermediate-, and high-risk, showing metastasis rates of 3.4%, 8.2%, and 26.3%, respectively.
The MMAI risk grouping system expands the population of men identified as having low metastatic risk and accurately pinpoints a high-risk subset with elevated metastasis rates. This approach aims to prevent both overtreatment and undertreatment in localized prostate cancer, facilitating shared decision making.
目前用于局限性前列腺癌的临床风险分层方法并不理想,导致过度治疗和治疗不足。最近,使用数字组织病理学的机器学习方法在 III 期试验中显示出了优越的预后能力。本研究旨在开发一种使用多模态人工智能 (MMAI) 模型的临床可用风险分组系统,该系统优于当前的国家综合癌症网络 (NCCN) 风险组。
该队列包括来自 NRG Oncology 八项随机 III 期试验的 9787 例局限性前列腺癌患者,他们接受了放射治疗、雄激素剥夺治疗和/或化疗。锁定的 MMAI 模型使用数字组织病理学图像和临床数据应用于每位患者。根据 10 年远处转移率分别为 3%和 10%,专家组就切点达成共识,将患者分为低危、中危和高危组。比较了 MMAI 的再分类和预后性能与三层次 NCCN 风险组。
对有censored 的患者进行的中位随访时间为 7.9 年。根据 NCCN 风险类别,30.4%的患者为低危,25.5%为中危,44.1%为高危。MMAI 风险分类将 43.5%的患者归为低危,34.6%归为中危,21.8%归为高危。MMAI 重新分类了 1039 名(42.0%)最初按 NCCN 分类的患者。尽管 MMAI 的低危组大于 NCCN 的低危组,但 10 年转移风险相当:NCCN 为 1.7%(95%CI,0.2 至 3.2),MMAI 为 3.2%(95%CI,1.7 至 4.7)。NCCN 高危患者的总体 10 年转移风险为 16.6%,而 MMAI 进一步将该组分为低危、中危和高危,转移率分别为 3.4%、8.2%和 26.3%。
MMAI 风险分组系统扩大了确定为低转移风险的男性人群,并准确地确定了具有较高转移率的高危亚组。这种方法旨在预防局限性前列腺癌的过度治疗和治疗不足,促进共同决策。