Esteva Andre, Feng Jean, van der Wal Douwe, Huang Shih-Cheng, Simko Jeffry P, DeVries Sandy, Chen Emmalyn, Schaeffer Edward M, Morgan Todd M, Sun Yilun, Ghorbani Amirata, Naik Nikhil, Nathawani Dhruv, Socher Richard, Michalski Jeff M, Roach Mack, Pisansky Thomas M, Monson Jedidiah M, Naz Farah, Wallace James, Ferguson Michelle J, Bahary Jean-Paul, Zou James, Lungren Matthew, Yeung Serena, Ross Ashley E, Sandler Howard M, Tran Phuoc T, Spratt Daniel E, Pugh Stephanie, Feng Felix Y, Mohamad Osama
Artera, Inc, Mountain View, CA, USA.
Department of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, CA, USA.
NPJ Digit Med. 2022 Jun 8;5(1):71. doi: 10.1038/s41746-022-00613-w.
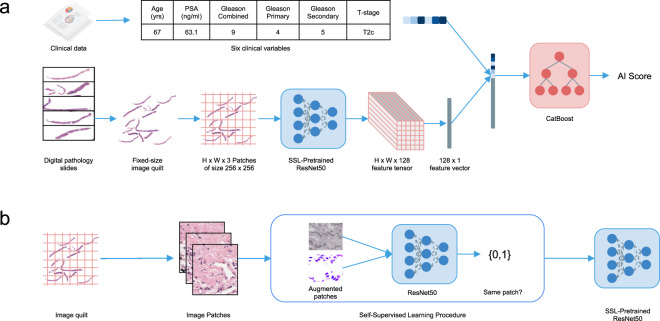
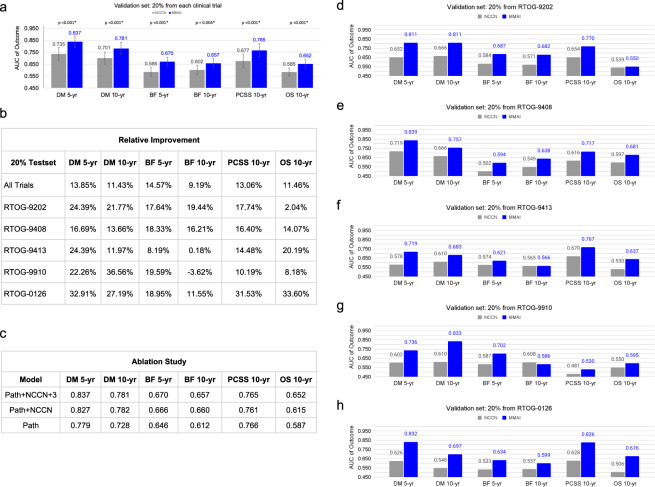
Prostate cancer is the most frequent cancer in men and a leading cause of cancer death. Determining a patient's optimal therapy is a challenge, where oncologists must select a therapy with the highest likelihood of success and the lowest likelihood of toxicity. International standards for prognostication rely on non-specific and semi-quantitative tools, commonly leading to over- and under-treatment. Tissue-based molecular biomarkers have attempted to address this, but most have limited validation in prospective randomized trials and expensive processing costs, posing substantial barriers to widespread adoption. There remains a significant need for accurate and scalable tools to support therapy personalization. Here we demonstrate prostate cancer therapy personalization by predicting long-term, clinically relevant outcomes using a multimodal deep learning architecture and train models using clinical data and digital histopathology from prostate biopsies. We train and validate models using five phase III randomized trials conducted across hundreds of clinical centers. Histopathological data was available for 5654 of 7764 randomized patients (71%) with a median follow-up of 11.4 years. Compared to the most common risk-stratification tool-risk groups developed by the National Cancer Center Network (NCCN)-our models have superior discriminatory performance across all endpoints, ranging from 9.2% to 14.6% relative improvement in a held-out validation set. This artificial intelligence-based tool improves prognostication over standard tools and allows oncologists to computationally predict the likeliest outcomes of specific patients to determine optimal treatment. Outfitted with digital scanners and internet access, any clinic could offer such capabilities, enabling global access to therapy personalization.
前列腺癌是男性中最常见的癌症,也是癌症死亡的主要原因。确定患者的最佳治疗方案是一项挑战,肿瘤学家必须选择成功可能性最高且毒性可能性最低的治疗方法。国际预后标准依赖于非特异性和半定量工具,通常会导致过度治疗和治疗不足。基于组织的分子生物标志物试图解决这一问题,但大多数在前瞻性随机试验中的验证有限且处理成本高昂,这对广泛应用构成了重大障碍。仍然迫切需要准确且可扩展的工具来支持个性化治疗。在此,我们通过使用多模态深度学习架构预测长期临床相关结果来展示前列腺癌治疗的个性化,并使用前列腺活检的临床数据和数字组织病理学来训练模型。我们使用在数百个临床中心进行的五项III期随机试验来训练和验证模型。在7764名随机分组的患者中,有5654名(71%)可获得组织病理学数据,中位随访时间为11.4年。与最常用的风险分层工具——美国国立综合癌症网络(NCCN)制定的风险组相比,我们的模型在所有终点上都具有更好的区分性能,在一个保留验证集中相对改善幅度从9.2%到14.6%不等。这种基于人工智能的工具比标准工具能更好地进行预后评估,并使肿瘤学家能够通过计算预测特定患者最可能的结果,以确定最佳治疗方案。配备数字扫描仪和互联网接入,任何诊所都可以提供这种能力,从而实现全球范围内的个性化治疗。