Coral Daniel E, Smit Femke, Farzaneh Ali, Gieswinkel Alexander, Tajes Juan Fernandez, Sparsø Thomas, Delfin Carl, Bauvin Pierre, Wang Kan, Temprosa Marinella, De Cock Diederik, Blanch Jordi, Fernández-Real José Manuel, Ramos Rafael, Ikram M Kamran, Gomez Maria F, Kavousi Maryam, Panova-Noeva Marina, Wild Philipp S, van der Kallen Carla, Adriaens Michiel, van Greevenbroek Marleen, Arts Ilja, Le Roux Carel, Ahmadizar Fariba, Frayling Timothy M, Giordano Giuseppe N, Pearson Ewan R, Franks Paul W
Genetic and Molecular Epidemiology Unit, Lund University Diabetes Centre, Department of Clinical Science, Lund University, Helsingborg, Sweden.
Maastricht Centre for Systems Biology (MaCSBio), Maastricht University, Maastricht, The Netherlands.
Nat Med. 2025 Feb;31(2):534-543. doi: 10.1038/s41591-024-03299-7. Epub 2024 Oct 24.
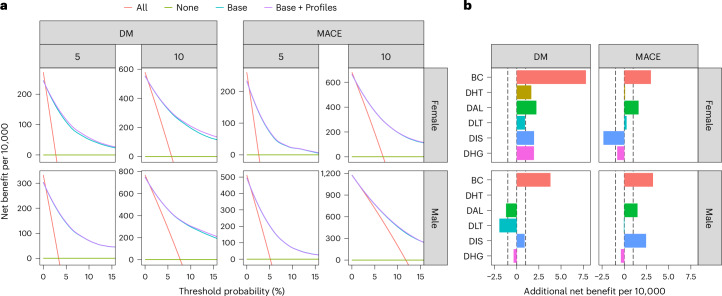
Obesity and cardiometabolic disease often, but not always, coincide. Distinguishing subpopulations within which cardiometabolic risk diverges from the risk expected for a given body mass index (BMI) may facilitate precision prevention of cardiometabolic diseases. Accordingly, we performed unsupervised clustering in four European population-based cohorts (N ≈ 173,000). We detected five discordant profiles consisting of individuals with cardiometabolic biomarkers higher or lower than expected given their BMI, which generally increases disease risk, in total representing ~20% of the total population. Persons with discordant profiles differed from concordant individuals in prevalence and future risk of major adverse cardiovascular events (MACE) and type 2 diabetes. Subtle BMI-discordances in biomarkers affected disease risk. For instance, a 10% higher probability of having a discordant lipid profile was associated with a 5% higher risk of MACE (hazard ratio in women 1.05, 95% confidence interval 1.03, 1.06, P = 4.19 × 10; hazard ratio in men 1.05, 95% confidence interval 1.04, 1.06, P = 9.33 × 10). Multivariate prediction models for MACE and type 2 diabetes performed better when incorporating discordant profile information (likelihood ratio test P < 0.001). This enhancement represents an additional net benefit of 4-15 additional correct interventions and 37-135 additional unnecessary interventions correctly avoided for every 10,000 individuals tested.
肥胖与心血管代谢疾病常常(但并非总是)同时出现。区分心血管代谢风险与给定体重指数(BMI)预期风险不同的亚群,可能有助于精准预防心血管代谢疾病。因此,我们在四个基于欧洲人群的队列(N≈173,000)中进行了无监督聚类。我们检测到五种不一致的概况,由心血管代谢生物标志物高于或低于其BMI预期水平的个体组成,而BMI通常会增加疾病风险,这些个体总共占总人口的约20%。具有不一致概况的人与一致个体在主要不良心血管事件(MACE)和2型糖尿病的患病率及未来风险方面存在差异。生物标志物中细微的BMI不一致会影响疾病风险。例如,脂质概况不一致的概率每高出10%,MACE风险就会高出5%(女性风险比1.05,95%置信区间1.03, 1.06,P = 4.19×10;男性风险比1.05,95%置信区间1.04, 1.06,P = 9.33×10)。当纳入不一致概况信息时,MACE和2型糖尿病的多变量预测模型表现更佳(似然比检验P < 0.001)。对于每10,000名接受检测的个体,这种增强代表着额外的净收益,即多做出4 - 15次正确干预,并正确避免37 - 135次额外的不必要干预。