Department of Intensive Care Medicine, Maastricht University Medical Center + (Maastricht UMC+), P. Debyelaan 25, 6229 HX, Maastricht, the Netherlands.
Department of Intensive Care Medicine, Laurentius Ziekenhuis, Roermond, the Netherlands.
Sci Rep. 2024 Nov 1;14(1):26344. doi: 10.1038/s41598-024-70333-6.
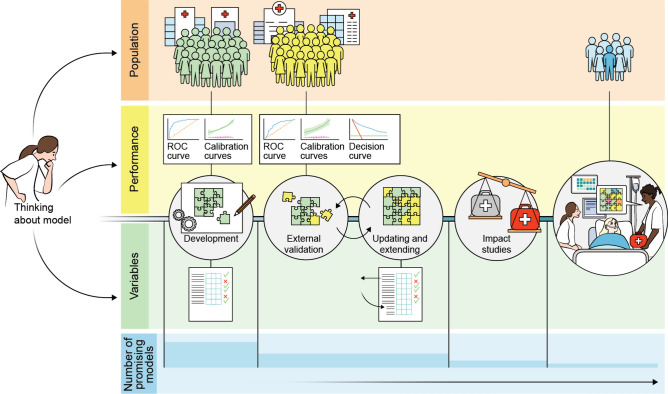
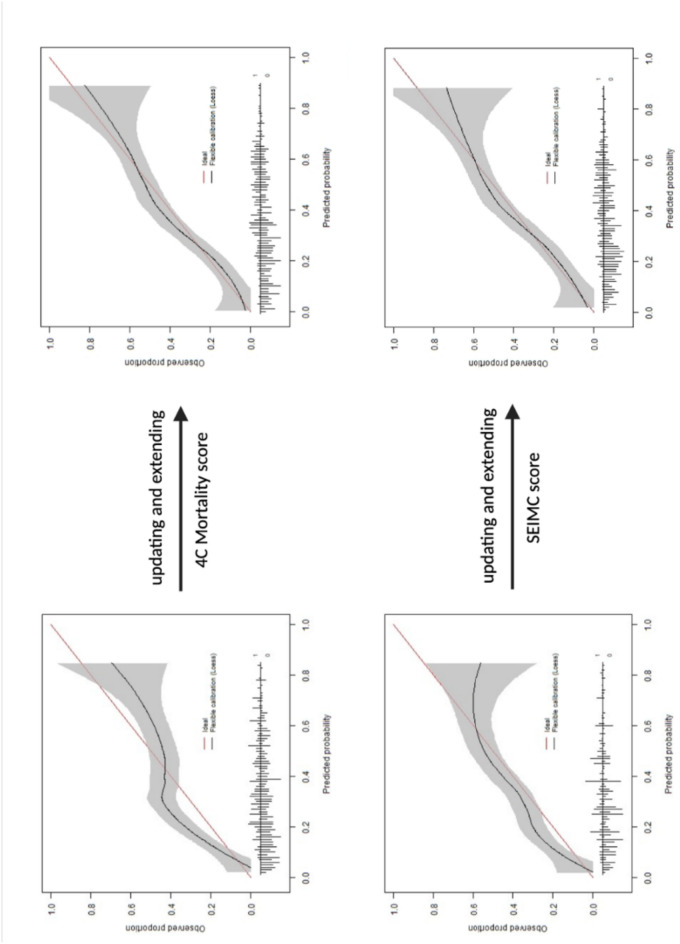
Most published prediction models for Coronavirus Disease 2019 (COVID-19) were poorly reported, at high risk of bias, and heterogeneous in model performance. To tackle methodological challenges faced in previous prediction studies, we investigated whether model updating and extending improves mortality prediction, using the Intensive Care Unit (ICU) as a proxy. All COVID-19 patients admitted to seven ICUs in the Euregio-Meuse Rhine during the first pandemic wave were included. The 4C Mortality and SEIMC scores were selected as promising prognostic models from an external validation study. Five predictors could be estimated based on cohort size. TRIPOD guidelines were followed and logistic regression analyses with the linear predictor, APACHE II score, and country were performed. Bootstrapping with backward selection was applied to select variables for the final model. Additionally, shrinkage was performed. Model discrimination was displayed as optimism-corrected areas under the ROC curve and calibration by calibration slopes and plots. The mortality rate of the 551 included patients was 36%. Discrimination of the 4C Mortality and SEIMC scores increased from 0.70 to 0.74 and 0.70 to 0.73 and calibration plots improved compared to the original models after updating and extending. Mortality prediction can be improved after updating and extending of promising models.
大多数发表的 2019 年冠状病毒病(COVID-19)预测模型报告不充分,存在较高的偏倚风险,且模型性能存在异质性。为了解决先前预测研究中面临的方法学挑战,我们研究了模型更新和扩展是否可以改善死亡率预测,以重症监护病房(ICU)作为替代。所有在第一次大流行期间在 Euregio-Meuse Rhine 地区的七个 ICU 住院的 COVID-19 患者均被纳入研究。4C 死亡率和 SEIMC 评分被选为来自外部验证研究的有前途的预后模型。可以根据队列大小估计五个预测因子。遵循 TRIPOD 指南,对线性预测因子、APACHE II 评分和国家进行逻辑回归分析。应用向后选择的自举法选择最终模型的变量。此外,还进行了收缩。通过校正后的 ROC 曲线下面积和校准斜率和图来显示模型的判别能力和校准。551 例纳入患者的死亡率为 36%。与原始模型相比,4C 死亡率和 SEIMC 评分的更新和扩展后,其判别能力从 0.70 提高到 0.74 和 0.70 提高到 0.73,校准图得到改善。对有前途的模型进行更新和扩展后,可以提高死亡率预测。