Department of Audiology, Sri Ramachandra Faculty of Audiiology and Speech Language Pathology, Sri Ramachandra Institute of Higher Education and Research (Deemed to be University), Chennai, Tamil Nadu, India.
Department of Audiology, Sri Ramachandra Faculty of Audiiology and Speech Language Pathology, Sri Ramachandra Institute of Higher Education and Research (Deemed to be University), Chennai, Tamil Nadu, India
BMJ Paediatr Open. 2024 Nov 5;8(1):e002794. doi: 10.1136/bmjpo-2024-002794.
Early Hearing Detection and Intervention (EHDI) programmes were established to reduce the impact of hearing loss on children. High-income countries (HICs) have resources and knowledge to execute these programmes. However, financial and other resource constraints limit the availability of these programmes to low-income and middle-income countries (LMICs). Yet, LMICs have explored strategies to implement EHDI programmes in their context; the outcomes are still largely unknown.The aim of this study is to identify the various models of the EHDI program implemented in non-Asian LMICs.
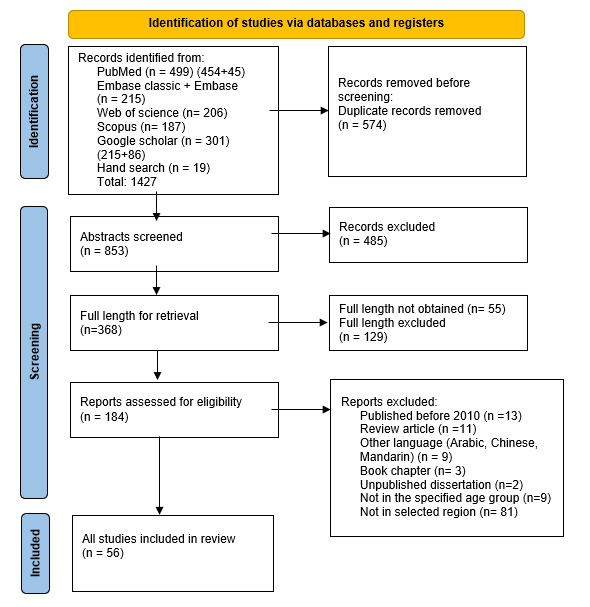
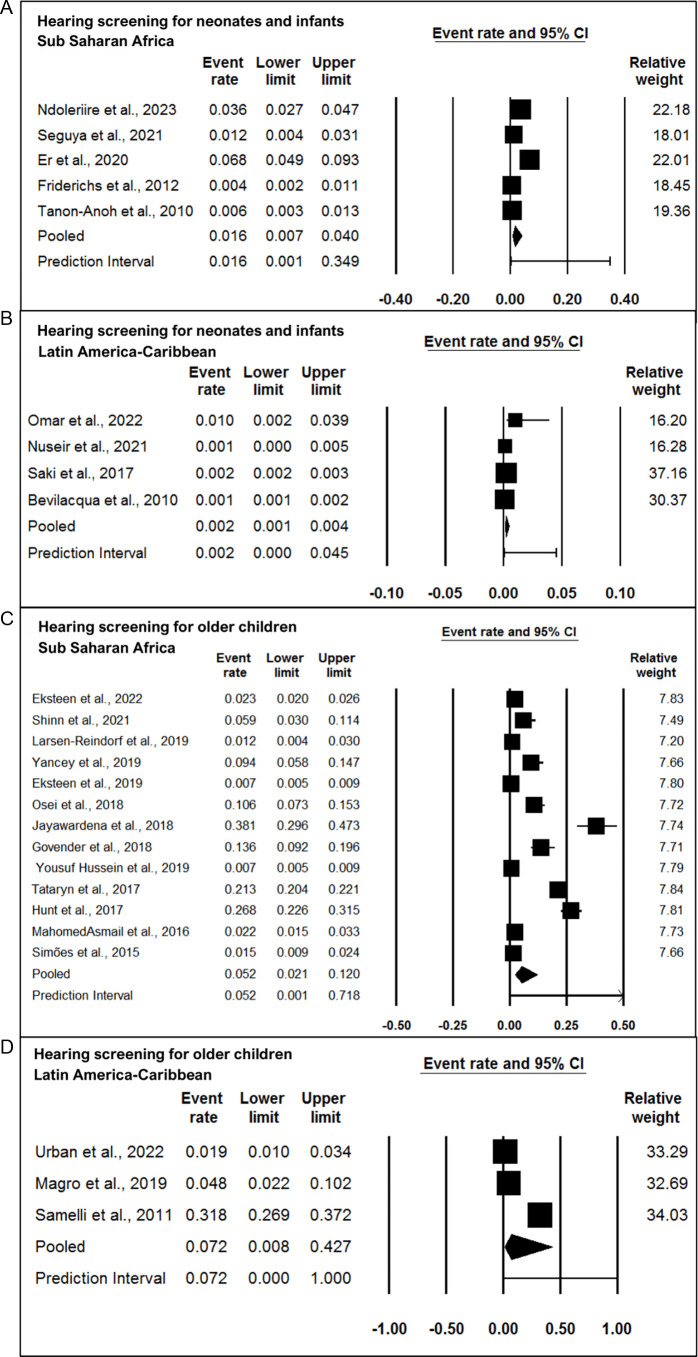
METHOD: Studies published between 2010 and 2023 reporting EHDI programmes in non-Asian LMICs for children were considered. The primary databases searched were PubMed, Scopus, Web of Science, EBSCOHost, EBSCO-CINAHL and ProQuest dissertations. The search results are summarised using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses chart. Quality appraisal and risk-of-bias assessment were assessed. Using the retrieved data, a narrative synthesis of the identified methods and forest plots for the prevalence estimate was created.
Fifty-six studies from 16 LMICs were included. They were grouped into 29 hearing screening programmes for neonates and infants and 26 programmes for older children. Predominantly hospital-based screening was employed for neonates and infants and school-based screening for older children. Two-stage otoacoustic emissions screening was employed for neonates and infants, while single-stage pure tone audiometry with otoscopy screening was used for older children. Predominantly, audiologists performed screening and diagnostics for neonates/infants while community health workers performed screening for the older children. Screening aspects were reported predominantly and not diagnostic evaluation/intervention outcomes. Overall, the economics of EHDI was reported only anecdotally in a few studies.
The screening strategies were not uniform among non-Asian LMICs. The protocols used were similar to HICs, yet few developed protocols adapting the Joint Committee of Infant Hearing. However, long-term outcomes such as rate of identification, suitable intervention and their outcomes are not known. EHDI programmes with successful outcomes of early intervention must be studied and reported with economic evaluations.
早期听力检测和干预 (EHDI) 计划的设立旨在减轻听力损失对儿童的影响。高收入国家 (HIC) 拥有执行这些计划的资源和知识。然而,财务和其他资源限制了这些计划在低收入和中等收入国家 (LMIC) 的可用性。然而,LMIC 已经探索了在其背景下实施 EHDI 计划的策略;结果在很大程度上仍然未知。本研究的目的是确定在非亚洲 LMIC 中实施的 EHDI 计划的各种模式。
方法:考虑了 2010 年至 2023 年期间发表的报告非亚洲 LMIC 中儿童 EHDI 计划的研究。主要搜索的数据库是 PubMed、Scopus、Web of Science、EBSCOHost、EBSCO-CINAHL 和 ProQuest 论文。使用系统评价和荟萃分析图表的首选报告项目总结搜索结果。进行了质量评估和风险偏倚评估。使用检索到的数据,创建了已识别方法的叙述性综合和流行率估计的森林图。
来自 16 个 LMIC 的 56 项研究被纳入。它们被分为 29 个新生儿和婴儿听力筛查计划和 26 个大龄儿童筛查计划。新生儿和婴儿主要采用基于医院的筛查,大龄儿童采用基于学校的筛查。新生儿和婴儿采用两阶段耳声发射筛查,大龄儿童采用单阶段纯音听力测试和耳镜筛查。主要由听力学家对新生儿/婴儿进行筛查和诊断,而由社区卫生工作者对大龄儿童进行筛查。主要报告了筛查方面,而不是诊断评估/干预结果。总体而言,只有少数研究偶然报告了 EHDI 的经济学。
非亚洲 LMIC 之间的筛查策略并不统一。使用的方案与 HIC 相似,但很少有方案采用联合婴儿听力委员会制定的方案。然而,长期结果,如识别率、合适的干预及其结果尚不清楚。必须研究和报告具有成功早期干预结果的 EHDI 计划,并进行经济评估。