Li Xunhua, Liu Qi, Dong Jingjie, Hong Yaonan, Xin Chuanao, Guo Junfeng, Liu Shan, Wang Peicheng, Sun Zexing, Shen Yingying, Yang Xiawan, Li Hangchao, Shen Yiping, Shen Jianping, Ye Baodong, Zhou Yuhong, Hu Tonglin, Wu Dijiong
Department of Nursing, Chuzhou City Vocational College, Chuzhou Anhui, China.
Department of Hematology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, China.
Ann Med. 2025 Dec;57(1):2446689. doi: 10.1080/07853890.2024.2446689. Epub 2024 Dec 28.
Platelet transfusion refractoriness (PTR) is a frustrating clinical problem, and primary and persistent (P/P) PTR who experienced persistent PTR since the first transfusion was failed to be well recognized. This study aims to investigate the incidence and risk factors for P/P PTR.
Patients with hematologic disorders who underwent HLA high-resolution genotyping and donor-specific HLA antibody or panel reactive antibody (PRA) testing between January 2019 and March 2023 were reviewed. Clinical data including infection history, splenomegaly, frequency and quantity of blood transfusions, and transfusions response were delineated and subsequently analyzed.
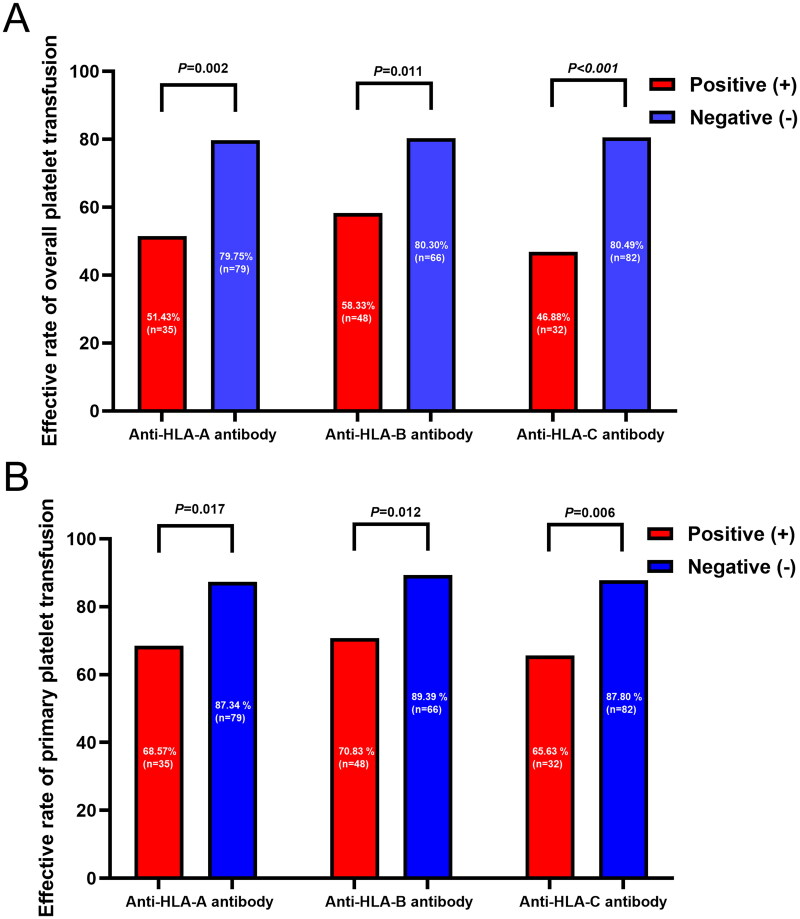
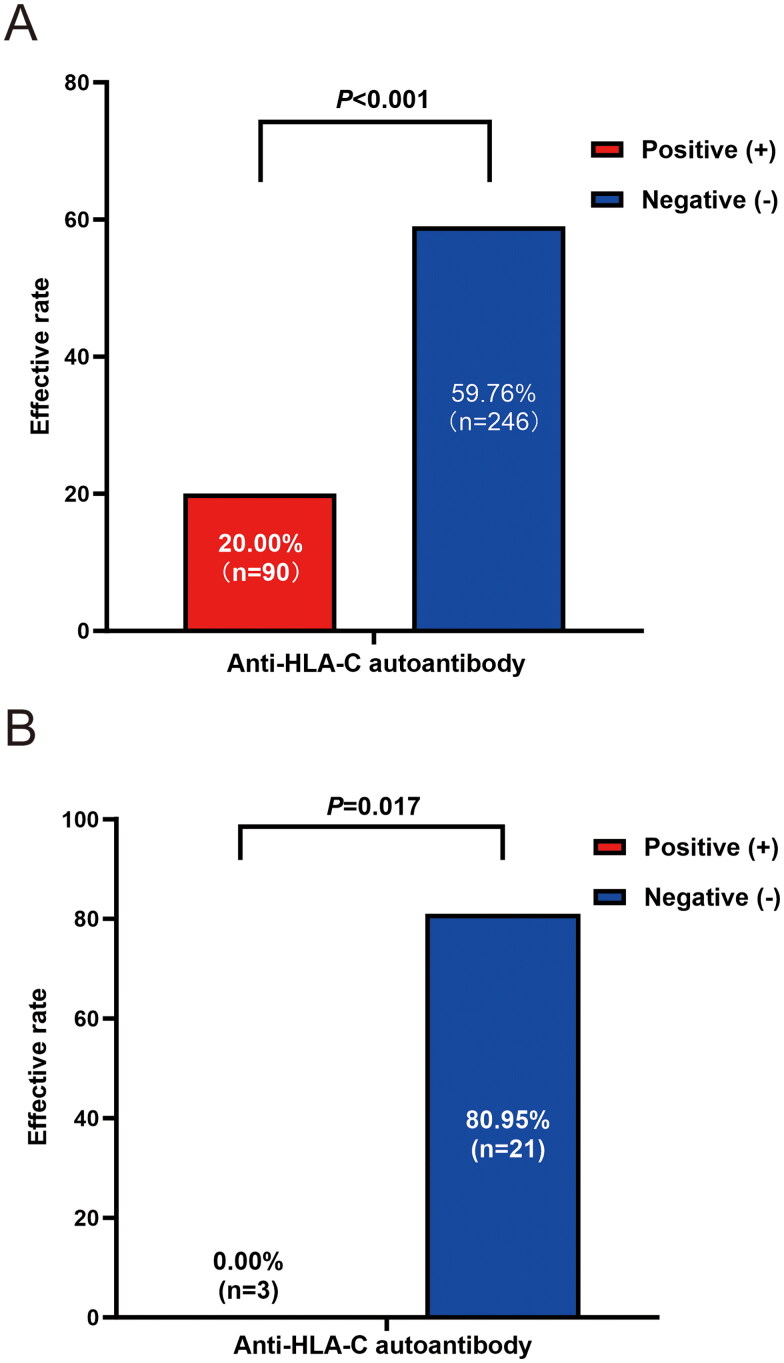
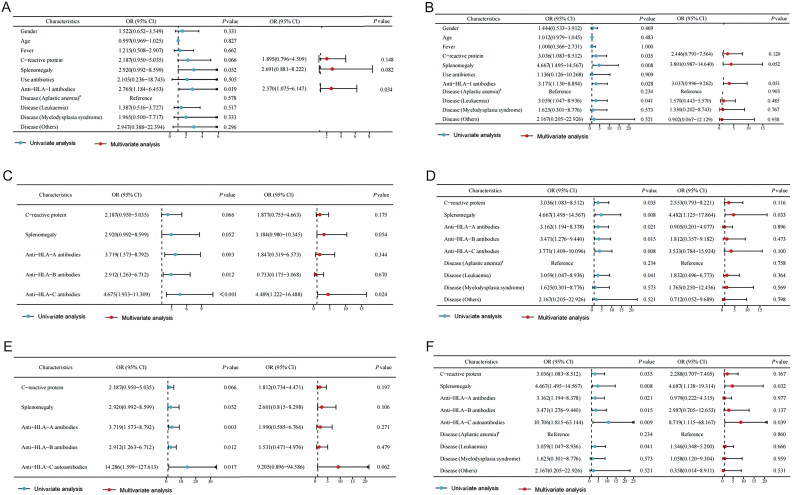
114 patients were included retrospectively, and 1071 transfusions were recorded. The overall incidence of PTR was 28.95% (33/114), with 63.63% (21/33) being P/P PTR. Anti class I HLA (anti-HLA-I) antibody was identified as an independent risk factor for ineffective platelet transfusion through multivariate logistic regression analysis ( = .034). Interestingly, anti-HLA-C autoantibodies were first found in six patients, and both anti-HLA-A and C autoantibodies were detected in one case, comprising a total of 10.71% (6/56) of HLA-I antibody-positive patients. Further analysis revealed that anti-HLA-C autoantibody was identified as an independent risk factor for P/P PTR ( = .039). Among patients with positive anti-HLA-C antibodies, significant differences in the effectiveness of ABO, D-matched and cross-matching transfusions were observed between patients with or without anti-HLA-C autoantibodies ( < .001 and = .017). Notably, platelet transfusions independence was achieved by two of the four patients who received rituximab.
This work emphasized the significance of anti-HLA-C autoantibody for P/P PTR in hematological patients, and rituximab may therapeutic.
血小板输注无效(PTR)是一个令人困扰的临床问题,而首次输血失败后即经历持续性PTR的原发性和持续性(P/P)PTR尚未得到充分认识。本研究旨在调查P/P PTR的发生率及危险因素。
回顾性分析2019年1月至2023年3月期间接受HLA高分辨率基因分型及供者特异性HLA抗体或群体反应性抗体(PRA)检测的血液系统疾病患者。描述包括感染史、脾肿大、输血频率和数量以及输血反应等临床数据,随后进行分析。
回顾性纳入114例患者,记录了1071次输血。PTR的总体发生率为28.95%(33/114),其中63.63%(21/33)为P/P PTR。通过多因素逻辑回归分析,抗I类HLA(抗-HLA-I)抗体被确定为血小板输注无效的独立危险因素(P = 0.034)。有趣的是,首次在6例患者中发现了抗-HLA-C自身抗体,1例患者同时检测到抗-HLA-A和C自身抗体,占HLA-I抗体阳性患者的10.71%(6/56)。进一步分析显示,抗-HLA-C自身抗体被确定为P/P PTR的独立危险因素(P = 0.039)。在抗-HLA-C抗体阳性的患者中,有或无抗-HLA-C自身抗体的患者在ABO、D配型和交叉配血输血有效性方面存在显著差异(P < 0.001和P = 0.017)。值得注意的是,接受利妥昔单抗治疗的4例患者中有2例实现了血小板输注独立。
本研究强调了抗-HLA-C自身抗体在血液系统疾病患者P/P PTR中的重要性,利妥昔单抗可能具有治疗作用。