Kodera Toshiaki, Isozaki Makoto, Kawajiri Satoshi, Yamada Shinsuke, Yamauchi Takahiro, Arishima Hidetaka, Kikuta Kenichiro
Department of Neurosurgery, University of Fukui, Fukui, JPN.
Cureus. 2024 Dec 2;16(12):e74950. doi: 10.7759/cureus.74950. eCollection 2024 Dec.
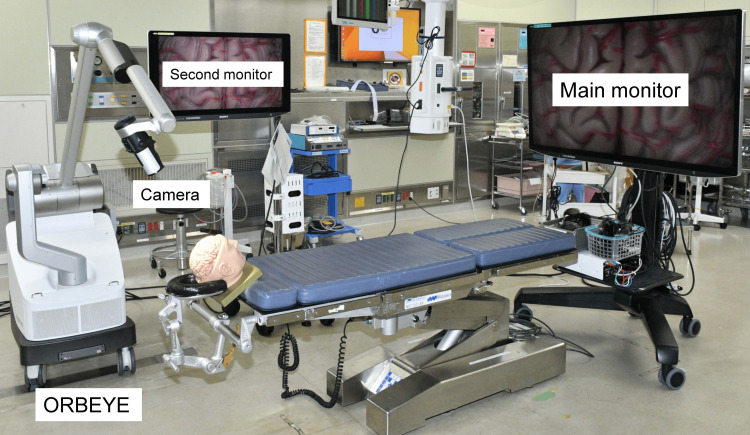
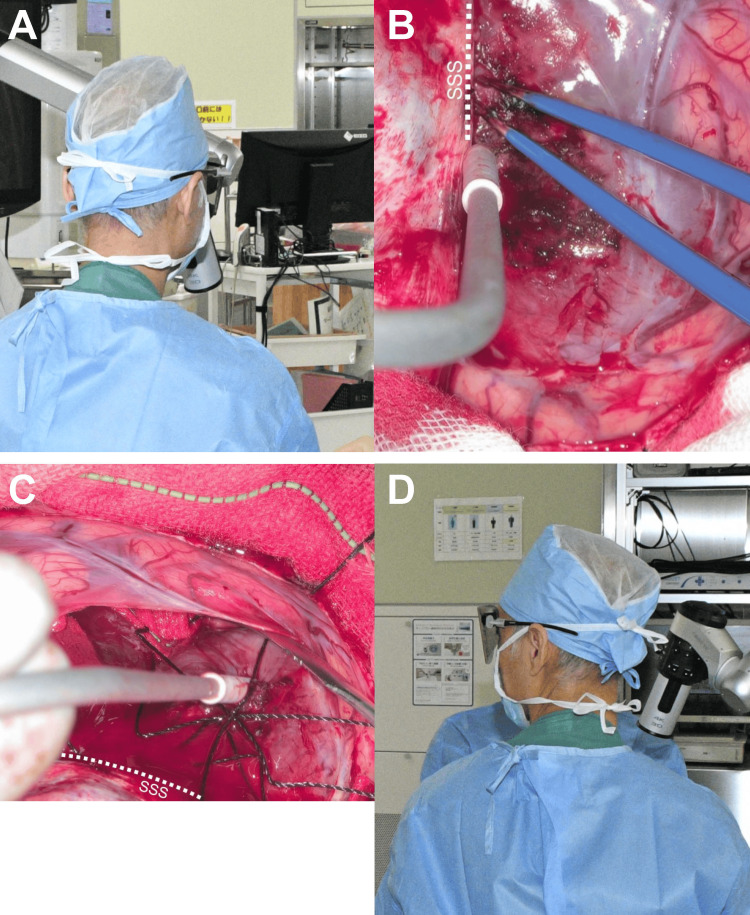
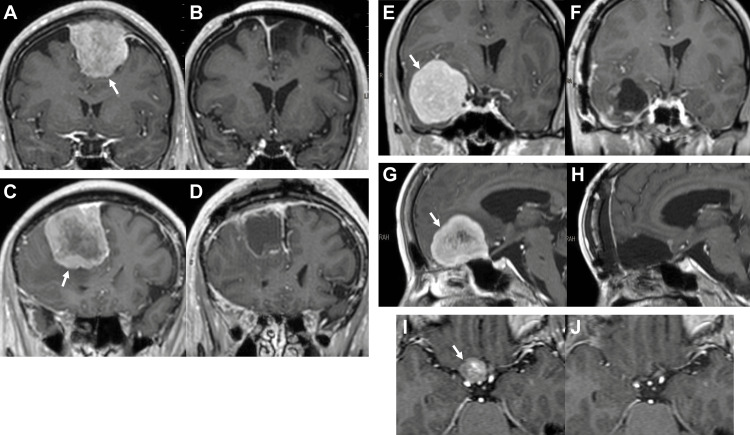
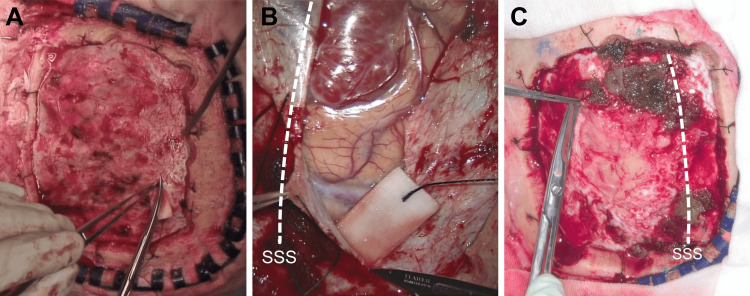
Background Prior to using the exoscope, we speculated that it represented an intermediate tool between a loupe and a microscope and had concerns about its visibility of deep, fine structures. Objective To evaluate the depths of meningioma for which the exoscope was suitable, and to clarify its disadvantages in meningioma resection. Methods Findings of consecutive meningioma surgeries using a 4K three-dimensional (3D) exoscope over a one-year period were evaluated for visibility of the surgical field, comfort of the surgeon's arm posture, the surgeon's head orientation, and perception of the image delay, accounting for the depth of the tumor. Results Seven meningiomas were resected using a 4K 3D exoscope (three superficial, three intermediate, and one deep). The exoscope allowed the surgeon to observe deeply located fine structures as clearly as with a conventional microscope and to operate more comfortably on meningiomas of all depths with arms flexed. On the contrary, the exoscope occasionally required the surgeon to operate with his head unnaturally turned to one side because of the immobility of its large monitor, despite the wide insertion availability of its camera from various directions to meningiomas located superficially or within the middle cranial fossa. No time delays between the surgeon's manipulations and the 3D images were perceived in all meningioma surgeries. Conclusions The 4K 3D exoscope was suitable for operations on all depths of meningiomas. The discrepancy between the surgeon's manipulation and gaze directions was its disadvantage. It is anticipated that further development of the 3D monitor will address this issue.
背景 在使用电子内镜之前,我们推测它是放大镜和显微镜之间的一种中间工具,并对其深部精细结构的可视性存在担忧。目的 评估电子内镜适用于的脑膜瘤深度,并阐明其在脑膜瘤切除术中的缺点。方法 对连续一年使用4K三维(3D)电子内镜进行的脑膜瘤手术的结果进行评估,包括手术视野的可视性、外科医生手臂姿势的舒适度、外科医生头部的方向以及图像延迟的感知,并考虑肿瘤的深度。结果 使用4K 3D电子内镜切除了7例脑膜瘤(3例浅表型、3例中间型和1例深部型)。电子内镜使外科医生能够像使用传统显微镜一样清晰地观察深部精细结构,并且在手臂弯曲的情况下,对外科医生操作各种深度的脑膜瘤都更舒适。相反,尽管其摄像头可以从各个方向广泛插入浅表或中颅窝内的脑膜瘤,但由于其大型显示器无法移动,电子内镜偶尔会要求外科医生不自然地将头转向一侧进行操作。在所有脑膜瘤手术中,均未察觉到外科医生操作与3D图像之间存在时间延迟。结论 4K 3D电子内镜适用于各种深度脑膜瘤的手术。外科医生操作方向与注视方向之间的差异是其缺点。预计3D显示器的进一步发展将解决这个问题。