Li Xiao-Han, Yang Xing-Long, Dong Bin-Bin, Liu Qi
Department of Emergency Intensive Care Unit, The First Affiliated Hospital of Zhengzhou University, No.1st, Jian She Eastern Road, Zhengzhou, 450052, Henan Province, People's Republic of China.
Faculty of Medicine, Khon Kaen University, No 123, Mittraphap Road, Khon Kaen, 40002, Thailand.
Cardiovasc Diabetol. 2025 Jan 8;24(1):10. doi: 10.1186/s12933-025-02577-z.
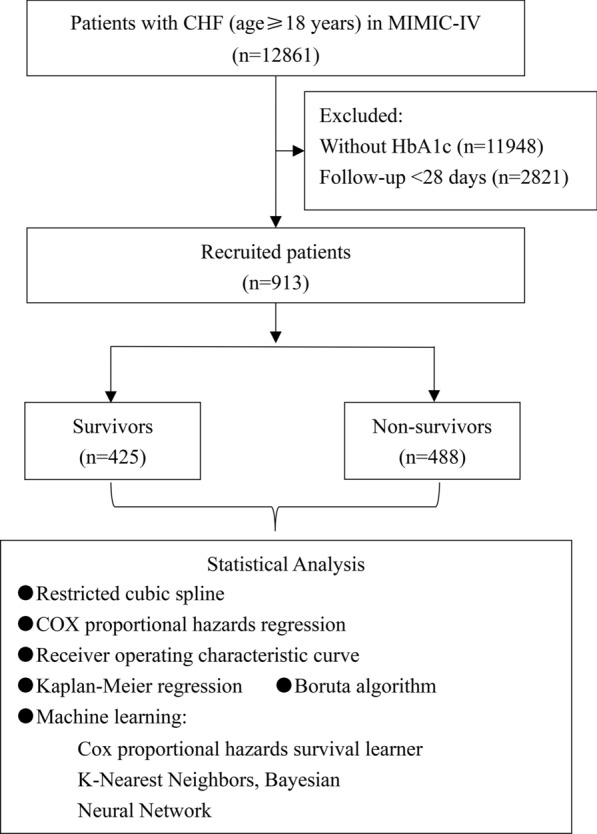
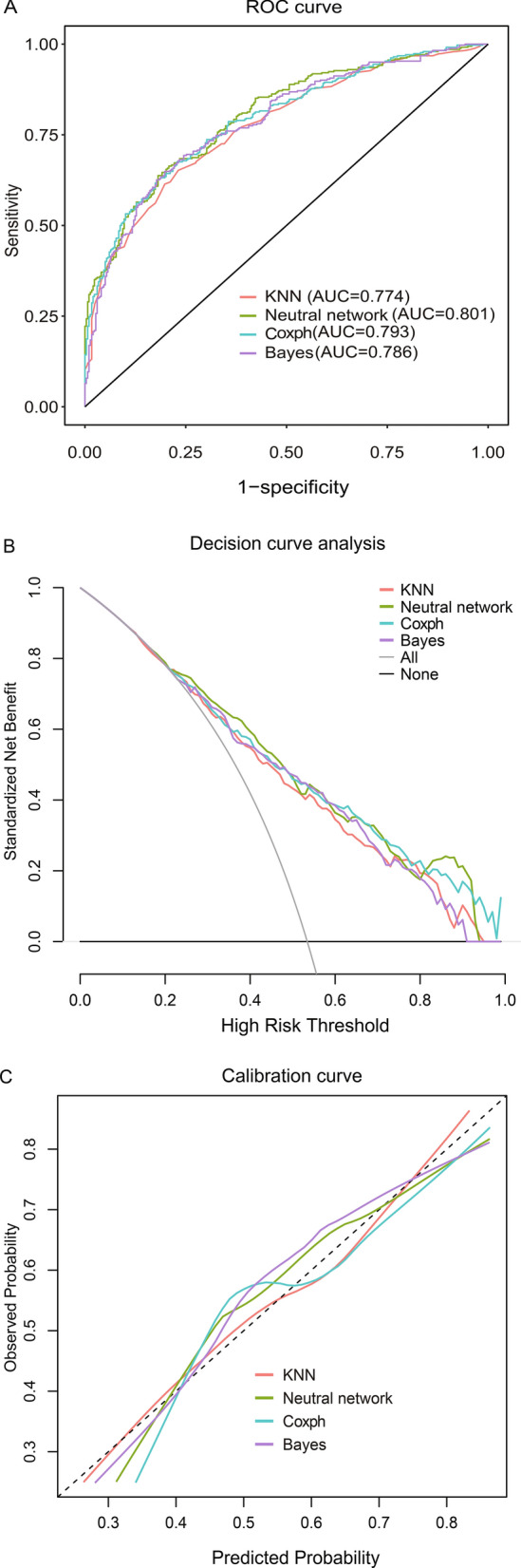
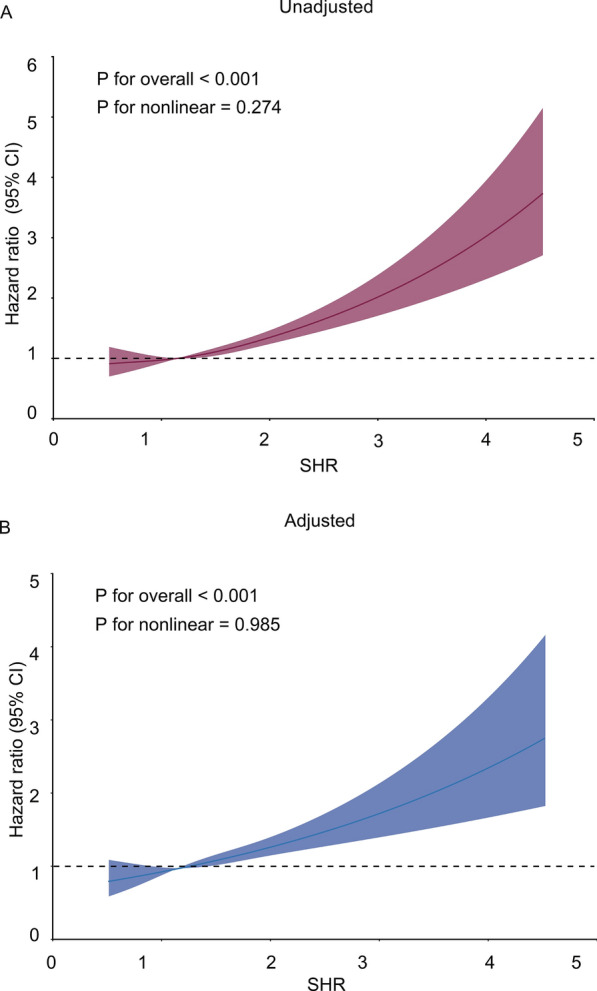
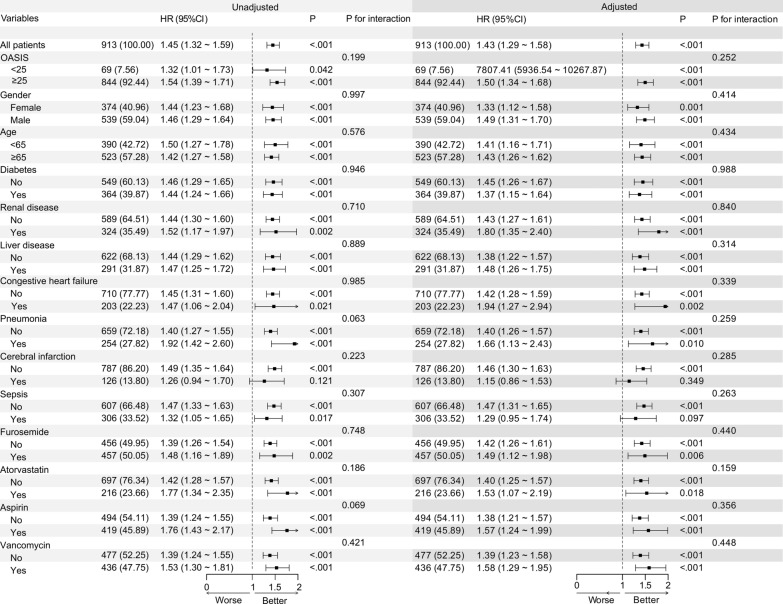
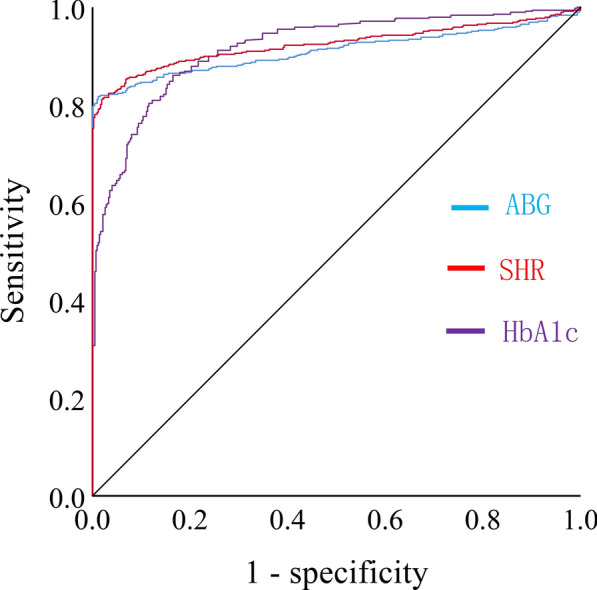
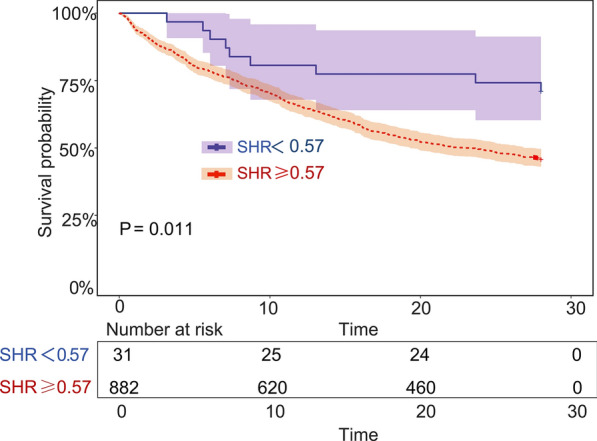
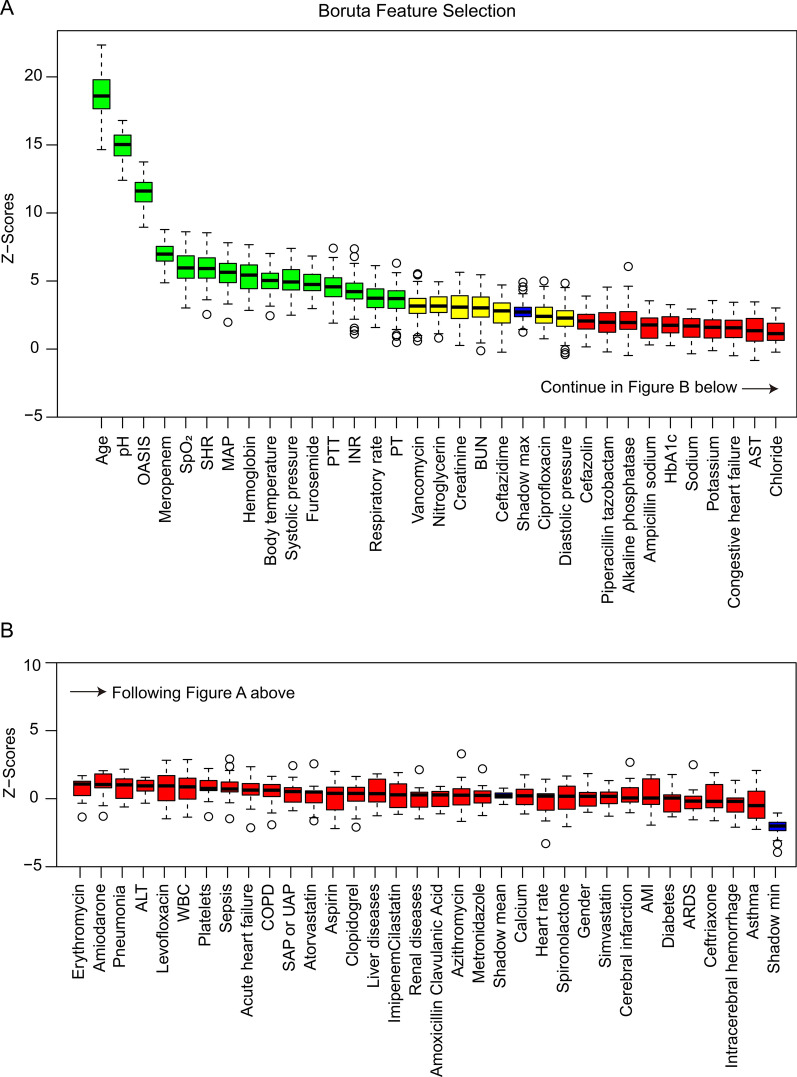
Chronic heart failure (CHF) poses a significant threat to human health. The stress hyperglycemia ratio (SHR) is a novel metric for accurately assessing stress hyperglycemia, which has been correlated with adverse outcomes in various major diseases. However, it remains unclear whether SHR is associated with 28-day mortality in patients with pre-existing CHF who were admitted to intensive care units (ICUs). This study retrospectively recruited patients who were admitted to ICUs with both acute critical illness and pre-existing CHF from the Medical Information Mart for Intensive Care (MIMIC) database. Characteristics were compared between the survival and non-survival groups. The relationship between SHR and 28-day all-cause mortality was analyzed using restricted cubic splines, receiver operating characteristic (ROC) curves, Kaplan-Meier survival analysis, and Cox proportional hazards regression analysis. The importance of the potential risk factors was assessed using the Boruta algorithm. Prediction models were constructed using machine learning algorithms. A total of 913 patients were enrolled. The risk of 28-day mortality increased with higher SHR levels (P < 0.001). SHR was independently associated with 28-day all-cause mortality, with an unadjusted hazard ratio (HR) of 1.45 (P < 0.001) and an adjusted HR of 1.43 (P < 0.001). Subgroup analysis found that none of the potential risk factors, such as demographics, comorbidities, and drugs, affected the relationship (P for interaction > 0.05). The area under the ROC (AUC) curve for SHR was larger than those for admission blood glucose and HbA1c; the cut-off for SHR was 0.57. Patients with SHR higher than the cut-off had a significantly lower 28-day survival probability (P < 0.001). SHR was identified as one of the key factors for 28-day mortality by the Boruta algorithm. The predictive performance was verified through four machine learning algorithms, with the neural network algorithm being the best (AUC 0.801). For patients with both acute critical illness and pre-existing CHF, SHR was an independent predictor of 28-day all-cause mortality. Its prognostic performance surpasses those of HbA1c and blood glucose, and prognostic models based on SHR provide clinicians with an effective tool to make therapeutic decisions.
慢性心力衰竭(CHF)对人类健康构成重大威胁。应激高血糖比(SHR)是一种用于准确评估应激性高血糖的新指标,它已与各种重大疾病的不良预后相关。然而,对于入住重症监护病房(ICU)的既往有CHF的患者,SHR是否与28天死亡率相关仍不清楚。本研究从重症监护医学信息集市(MIMIC)数据库中回顾性招募了因急性危重症和既往有CHF而入住ICU的患者。比较了生存组和非生存组的特征。使用受限立方样条、受试者工作特征(ROC)曲线、Kaplan-Meier生存分析和Cox比例风险回归分析来分析SHR与28天全因死亡率之间的关系。使用Boruta算法评估潜在风险因素的重要性。使用机器学习算法构建预测模型。共纳入913例患者。28天死亡率风险随SHR水平升高而增加(P < 0.001)。SHR与28天全因死亡率独立相关,未调整的风险比(HR)为1.45(P < 0.001),调整后的HR为1.43(P < 0.001)。亚组分析发现,人口统计学、合并症和药物等潜在风险因素均未影响这种关系(交互作用P > 0.05)。SHR的ROC曲线下面积(AUC)大于入院血糖和糖化血红蛋白的AUC;SHR的临界值为0.57。SHR高于临界值的患者28天生存概率显著较低(P < 0.001)。通过Boruta算法确定SHR是28天死亡率的关键因素之一。通过四种机器学习算法验证了预测性能,其中神经网络算法最佳(AUC 0.801)。对于患有急性危重症和既往有CHF的患者,SHR是28天全因死亡率的独立预测因子。其预后性能优于糖化血红蛋白和血糖,基于SHR的预后模型为临床医生提供了一个有效的治疗决策工具。