Barbeta Enric, Barreiros Cláudia, Forin Edoardo, Guzzardella Amedeo, Motos Anna, Fernández-Barat Laia, Gabarrús Albert, Ceccato Adrián, Ferrer Ricard, Riera Jordi, Peñuelas Oscar, Lorente José Ángel, de Gonzalo-Calvo David, Gonzalez Jessica, Amaya-Villar Rosario, Añón José Manuel, Balan Ana, Barberà Carme, Barberán José, Blandino Aaron, Boado Maria Victoria, Bustamante-Munguira Elena, Caballero Jesús, Cantón-Bulnes María Luisa, Carbajales Cristina, Carbonell Nieves, Catalán-González Mercedes, Franco Nieves, Galbán Cristóbal, Gumucio-Sanguino Víctor D, de la Torre Maria Del Carmen, Díaz Emilio, Estella Ángel, Gallego Elena, Gómez José Manuel, Huerta Arturo, García Ruth Noemí Jorge, Loza-Vázquez Ana, Marin-Corral Judith, Delgado María Cruz Martin, Martínez Amalia, Martínez Ignacio, Lopez Juan, Albaiceta Guillermo M, Nieto María Teresa, Novo Mariana Andrea, Peñasco Yhivian, Pérez-García Felipe, Ricart Pilar, Rodríguez Alejandro, Sagredo Victor, Sánchez-Miralles Angel, Sancho Susana, Roche-Campo Ferran, Socias Lorenzo, Solé-Violan Jordi, Tamayo Luis, Trenado José, Úbeda Alejandro, Valdivia Luis Jorge, Vidal Pablo, Barbé Ferran, Vallverdú Jordi, Torres Antoni
CIBER de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain.
Surgical Intensive Care Unit, Anesthesiology, Hospital Clinic of Barcelona, Barcelona, Spain.
Ann Intensive Care. 2025 Feb 25;15(1):27. doi: 10.1186/s13613-025-01430-6.
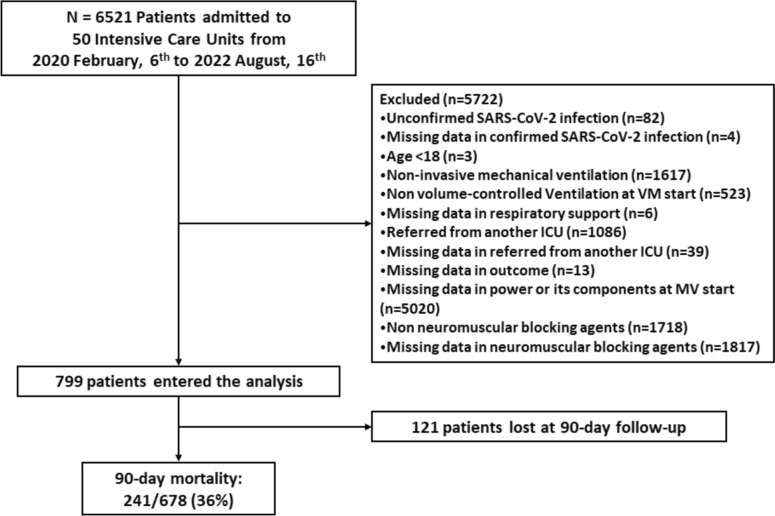
The relative contribution of the different components of mechanical power to mortality is a subject of debate and has not been studied in COVID-19. The aim of this study is to evaluate both the total and the relative impact of each of the components of mechanical power on mortality in a well-characterized cohort of patients with COVID-19-induced acute respiratory failure undergoing invasive mechanical ventilation. This is a secondary analysis of the CIBERESUCICOVID project, a multicenter observational cohort study including fifty Spanish intensive care units that included COVID-19 mechanically ventilated patients between February 2020 and December 2021. We examined the association between mechanical power and its components (elastic static, elastic dynamic, total elastic and resistive power) with 90-day mortality after adjusting for confounders in seven hundred ninety-nine patients with COVID-19-induced respiratory failure undergoing invasive mechanical ventilation.
At the initiation of mechanical ventilation, the PaO/FiO ratio was 106 (78; 150), ventilatory ratio was 1.69 (1.40; 2.05), and respiratory system compliance was 35.7 (29.2; 44.5) ml/cmHO. Mechanical power at the initiation of mechanical ventilation was 24.3 (18.9; 29.6) J/min, showing no significant changes after three days. In multivariable regression analyses, mechanical power and its components were not associated with 90-day mortality at the start of mechanical ventilation. After three days, total elastic and elastic static power were associated with higher 90-day mortality, but this relationship was also found for positive end-expiratory pressure.
Neither mechanical power nor its components were independently associated with mortality in COVID-19-induced acute respiratory failure at the start of MV. Nevertheless, after three days, static elastic power and total elastic power were associated with lower odds of survival. Positive end-expiratory pressure and plateau pressure, however, captured this risk in a similar manner.
机械功率不同组成部分对死亡率的相对贡献存在争议,且在新型冠状病毒肺炎(COVID-19)中尚未得到研究。本研究的目的是评估机械功率各组成部分对接受有创机械通气的COVID-19诱发急性呼吸衰竭患者队列中死亡率的总体和相对影响。这是对CIBERESUCICOVID项目的二次分析,该项目是一项多中心观察性队列研究,纳入了五十家西班牙重症监护病房,其中包括2020年2月至2021年12月期间接受机械通气的COVID-19患者。我们在对799例接受有创机械通气的COVID-19诱发呼吸衰竭患者的混杂因素进行校正后,研究了机械功率及其组成部分(弹性静态、弹性动态、总弹性和阻力功率)与90天死亡率之间的关联。
在机械通气开始时,动脉血氧分压/吸入氧浓度(PaO/FiO)比值为106(78;150),通气比为1.69(1.40;2.05),呼吸系统顺应性为35.7(29.2;44.5)ml/cmH₂O。机械通气开始时的机械功率为24.3(18.9;29.6)J/min,三天后无显著变化。在多变量回归分析中,机械通气开始时机械功率及其组成部分与90天死亡率无关。三天后,总弹性和弹性静态功率与较高的90天死亡率相关,但呼气末正压也存在这种关系。
在机械通气开始时,机械功率及其组成部分均与COVID-19诱发急性呼吸衰竭的死亡率无独立关联。然而,三天后,静态弹性功率和总弹性功率与较低的生存几率相关。然而,呼气末正压和平台压以类似方式反映了这种风险。