Ebell Mark H, Rahmatullah Ivan, Hulme Cassie, Buhr Michelle, Kotnik Jack Henry, Geyer Rachel, Thompson Matthew, Lutz Barry
Department of Family Medicine, Michigan State University, East Lansing, Michigan, USA
Universitas Airlangga, Surabaya, East Java, Indonesia.
BMJ Open. 2025 Mar 3;15(3):e067574. doi: 10.1136/bmjopen-2022-067574.
The objective of this study is to perform a comprehensive systematic review and meta-analysis of the accuracy of signs, symptoms and case definitions for the diagnosis of influenza.
Systematic review and meta-analysis of diagnostic accuracy.
Inpatient or outpatient setting.
Three databases (PubMed, CINAHL and EMBASE) were searched through February 2024 for studies of clinical diagnosis of influenza using prospective data collection and a high-quality reference standard. Data were abstracted by researchers working in parallel and resolving discrepancies by discussion.
Quality was assessed using QUADAS-2. Summary estimates (or ranges) of sensitivity and specificity, likelihood ratio (LR), the Youden Index and the area under the receiver operating characteristic curve were calculated.
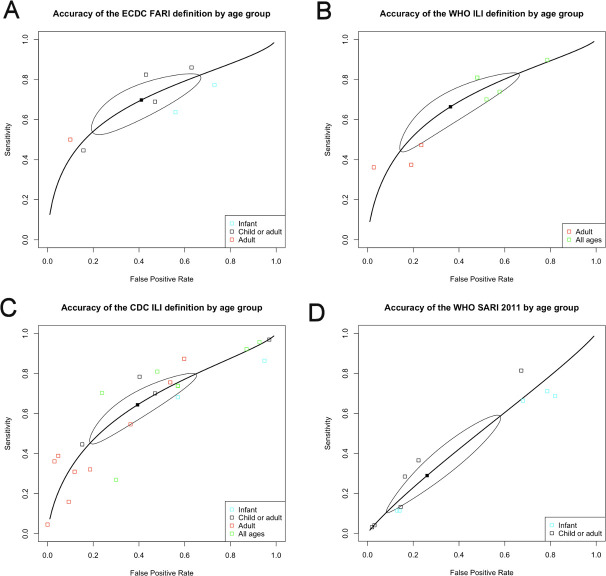
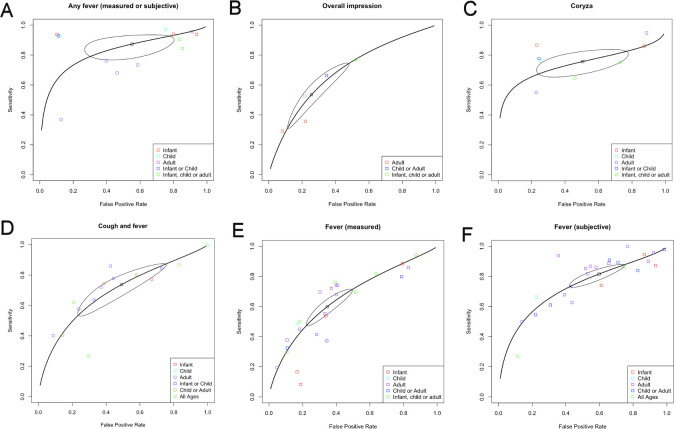
The final meta-analysis included 67 studies, each with between 119 and 155 866 participants. Most were judged to be low risk of bias. The signs and symptoms with the highest overall accuracy for all studies based on the Youden Index were any fever (0.32), overall clinical impression (0.28), coryza (0.25), cough and fever (0.25), and measured fever (0.25). Accuracy varied widely by age group. Only the overall clinical impression had a positive LR greater than 2.0. Cough was the most sensitive finding (0.92) with a negative LR of 0.28 in adults. The absence of any fever also had a low negative LR (0.30). The Centers for Disease Control and Prevention (CDC) definition of influenza-like illness (ILI) had good specificity but poor sensitivity in adults, while in infants, it had good sensitivity but widely varying specificity. The European CDC and WHO case definitions for ILI had modest sensitivity and specificity.
Individual signs and symptoms, their combinations, and ILI case definitions have very limited accuracy for identifying persons with influenza. More accurate surveillance and diagnosis will require the development and validation of accurate risk scores or greater use of point-of-care testing.
本研究的目的是对流感诊断的体征、症状及病例定义的准确性进行全面的系统评价和荟萃分析。
诊断准确性的系统评价和荟萃分析。
住院或门诊环境。
通过检索三个数据库(PubMed、CINAHL和EMBASE),直至2024年2月,查找使用前瞻性数据收集和高质量参考标准进行流感临床诊断的研究。数据由并行工作的研究人员提取,并通过讨论解决差异。
使用QUADAS-2评估质量。计算敏感性和特异性的汇总估计值(或范围)、似然比(LR)、约登指数和受试者工作特征曲线下面积。
最终的荟萃分析纳入了67项研究,每项研究的参与者人数在119至155866之间。大多数研究被判定为偏倚风险较低。基于约登指数,所有研究中总体准确性最高的体征和症状为任何发热(0.32)、总体临床印象(0.28)、鼻塞(0.25)、咳嗽伴发热(0.25)和实测发热(0.25)。准确性因年龄组而异。只有总体临床印象的阳性似然比大于2.0。咳嗽是最敏感的发现(0.92),成人的阴性似然比为0.28。无任何发热的阴性似然比也较低(0.30)。美国疾病控制与预防中心(CDC)对流感样疾病(ILI)的定义在成人中具有良好的特异性,但敏感性较差,而在婴儿中,其具有良好的敏感性,但特异性差异很大。欧洲疾病预防控制中心和世界卫生组织对ILI的病例定义具有中等的敏感性和特异性。
个体体征和症状、其组合以及ILI病例定义在识别流感患者方面的准确性非常有限。更准确的监测和诊断将需要开发和验证准确的风险评分或更多地使用即时检测。