Lancet. 2022 Jul 30;400(10349):359-368. doi: 10.1016/S0140-6736(22)01109-6.
We aimed to evaluate the use of baricitinib, a Janus kinase (JAK) 1-2 inhibitor, for the treatment of patients admitted to hospital with COVID-19.
This randomised, controlled, open-label, platform trial (Randomised Evaluation of COVID-19 Therapy [RECOVERY]), is assessing multiple possible treatments in patients hospitalised with COVID-19 in the UK. Eligible and consenting patients were randomly allocated (1:1) to either usual standard of care alone (usual care group) or usual care plus baricitinib 4 mg once daily by mouth for 10 days or until discharge if sooner (baricitinib group). The primary outcome was 28-day mortality assessed in the intention-to-treat population. A meta-analysis was done, which included the results from the RECOVERY trial and all previous randomised controlled trials of baricitinib or other JAK inhibitor in patients hospitalised with COVID-19. The RECOVERY trial is registered with ISRCTN (50189673) and ClinicalTrials.gov (NCT04381936) and is ongoing.
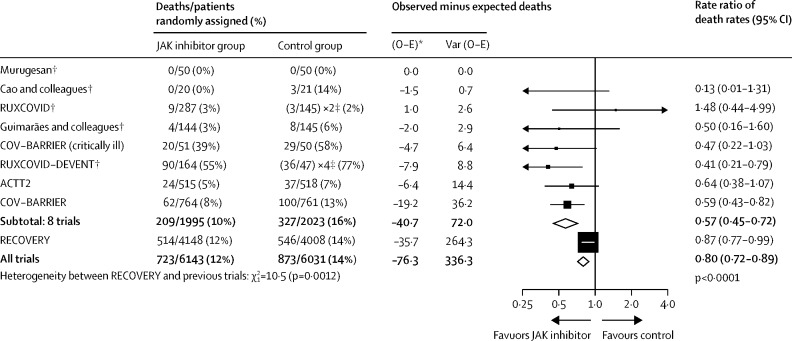
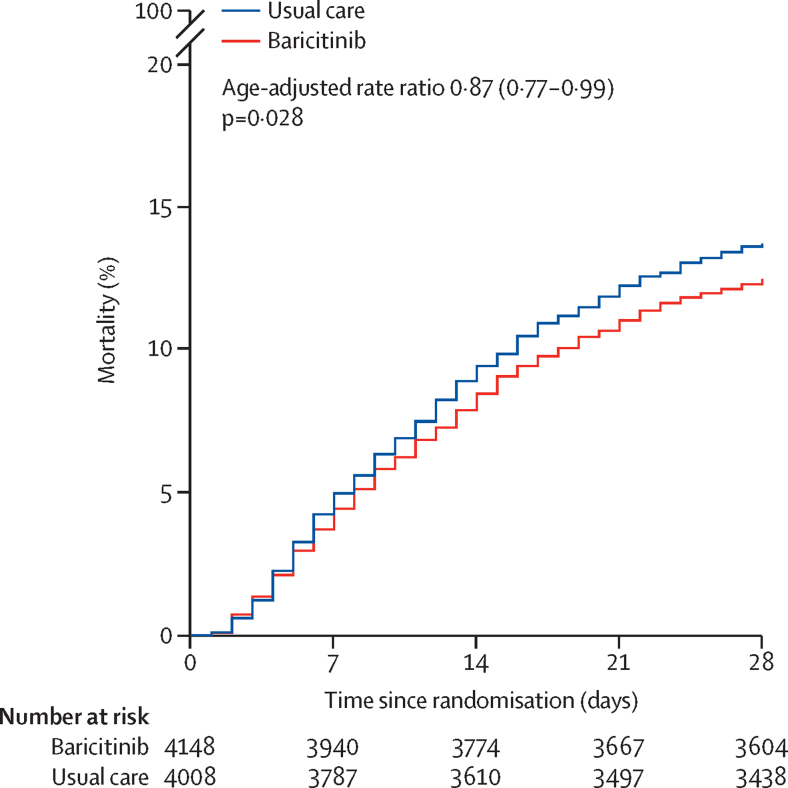
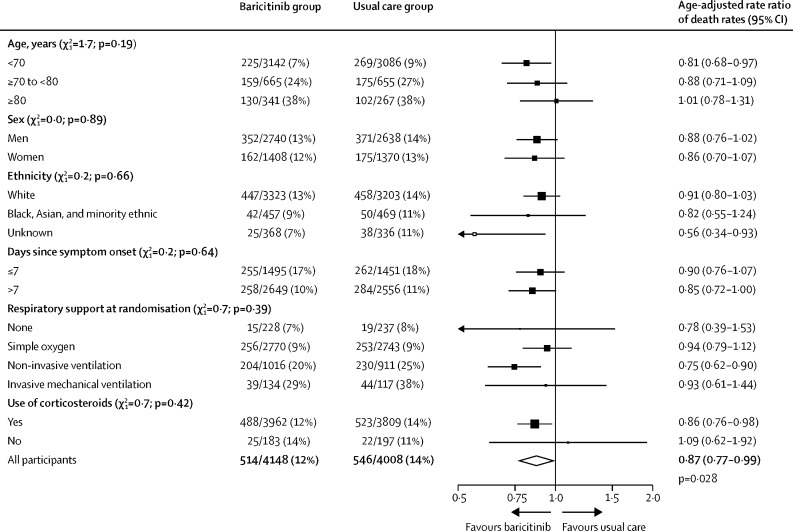
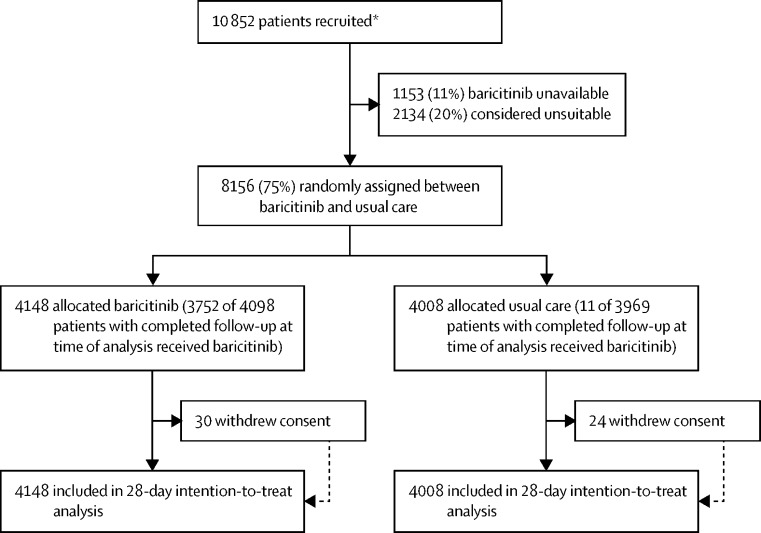
Between Feb 2 and Dec 29, 2021, from 10 852 enrolled, 8156 patients were randomly allocated to receive usual care plus baricitinib versus usual care alone. At randomisation, 95% of patients were receiving corticosteroids and 23% were receiving tocilizumab (with planned use within the next 24 h recorded for a further 9%). Overall, 514 (12%) of 4148 patients allocated to baricitinib versus 546 (14%) of 4008 patients allocated to usual care died within 28 days (age-adjusted rate ratio 0·87; 95% CI 0·77-0·99; p=0·028). This 13% proportional reduction in mortality was somewhat smaller than that seen in a meta-analysis of eight previous trials of a JAK inhibitor (involving 3732 patients and 425 deaths), in which allocation to a JAK inhibitor was associated with a 43% proportional reduction in mortality (rate ratio 0·57; 95% CI 0·45-0·72). Including the results from RECOVERY in an updated meta-analysis of all nine completed trials (involving 11 888 randomly assigned patients and 1485 deaths) allocation to baricitinib or another JAK inhibitor was associated with a 20% proportional reduction in mortality (rate ratio 0·80; 95% CI 0·72-0·89; p<0·0001). In RECOVERY, there was no significant excess in death or infection due to non-COVID-19 causes and no significant excess of thrombosis, or other safety outcomes.
In patients hospitalised with COVID-19, baricitinib significantly reduced the risk of death but the size of benefit was somewhat smaller than that suggested by previous trials. The total randomised evidence to date suggests that JAK inhibitors (chiefly baricitinib) reduce mortality in patients hospitalised for COVID-19 by about one-fifth.
UK Research and Innovation (Medical Research Council) and National Institute of Health Research.
我们旨在评估巴瑞替尼(一种 Janus 激酶 [JAK] 1-2 抑制剂)在治疗因 COVID-19 住院的患者中的应用。
这是一项随机、对照、开放性、平台试验(恢复研究),正在评估英国因 COVID-19 住院的患者中多种可能的治疗方法。符合条件并同意的患者以 1:1 的比例随机分配(随机分组)接受标准治疗(常规护理组)或标准治疗加每日口服巴瑞替尼 4 mg,持续 10 天或直至出院(巴瑞替尼组)。主要结局为在意向治疗人群中评估 28 天死亡率。进行了一项荟萃分析,其中包括恢复研究和之前所有关于巴瑞替尼或其他 JAK 抑制剂在因 COVID-19 住院的患者中的随机对照试验的结果。恢复研究在 ISRCTN(50189673)和 ClinicalTrials.gov(NCT04381936)注册,正在进行中。
在 2021 年 2 月 2 日至 12 月 29 日期间,从登记的 10852 名患者中,8156 名患者被随机分配接受常规护理加巴瑞替尼与常规护理单独治疗。随机分组时,95%的患者正在接受皮质类固醇治疗,23%的患者正在接受托珠单抗治疗(另有 9%计划在未来 24 小时内使用)。总体而言,在接受巴瑞替尼治疗的 4148 名患者中,有 514 名(12%)在 28 天内死亡,而在接受常规护理的 4008 名患者中,有 546 名(14%)死亡(年龄调整后的率比为 0.87;95%CI 0.77-0.99;p=0.028)。这种 13%的死亡率成比例降低略小于之前八项 JAK 抑制剂试验的荟萃分析(涉及 3732 名患者和 425 例死亡)中观察到的降低幅度,其中 JAK 抑制剂的分配与死亡率成比例降低 43%(率比为 0.57;95%CI 0.45-0.72)。将恢复研究的结果纳入所有九项已完成试验的更新荟萃分析(涉及 11888 名随机分配的患者和 1485 例死亡)中,巴瑞替尼或其他 JAK 抑制剂的分配与死亡率降低 20%相关(率比为 0.80;95%CI 0.72-0.89;p<0.0001)。在恢复研究中,因非 COVID-19 原因导致的死亡或感染没有显著增加,血栓形成或其他安全性结果也没有显著增加。
在因 COVID-19 住院的患者中,巴瑞替尼显著降低了死亡风险,但获益幅度略小于之前的试验提示的幅度。迄今为止,总随机证据表明,JAK 抑制剂(主要是巴瑞替尼)可使因 COVID-19 住院的患者的死亡率降低约五分之一。
英国研究与创新署(医学研究理事会)和英国国家卫生研究院。