Skrobisz Katarzyna, Miszewski Kevin, Miszewska Laura, Bieńkowski Michał, Matuszewski Marcin, Studniarek Michał
Department of Radiology, Medical University of Gdańsk, 17 Smoluchowskiego St., 80-214 Gdańsk, Poland.
Department of Urology, Medical University of Gdańsk, 17 Smoluchowskiego St., 80-214 Gdańsk, Poland.
Diagnostics (Basel). 2025 Mar 10;15(6):666. doi: 10.3390/diagnostics15060666.
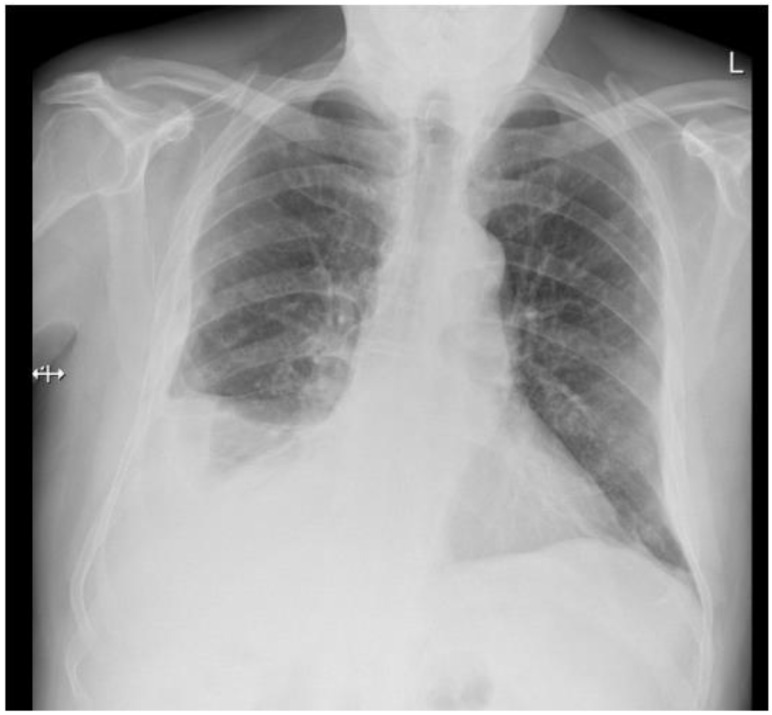
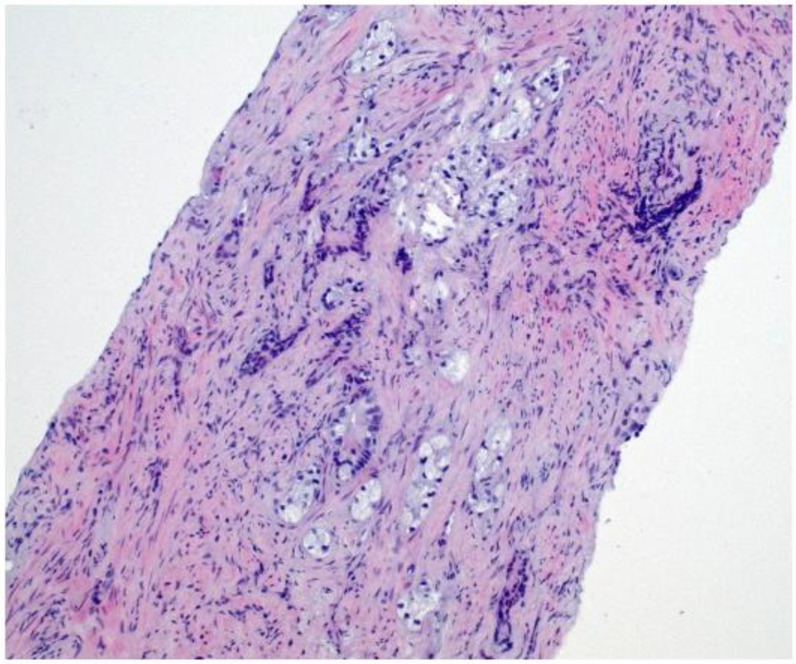
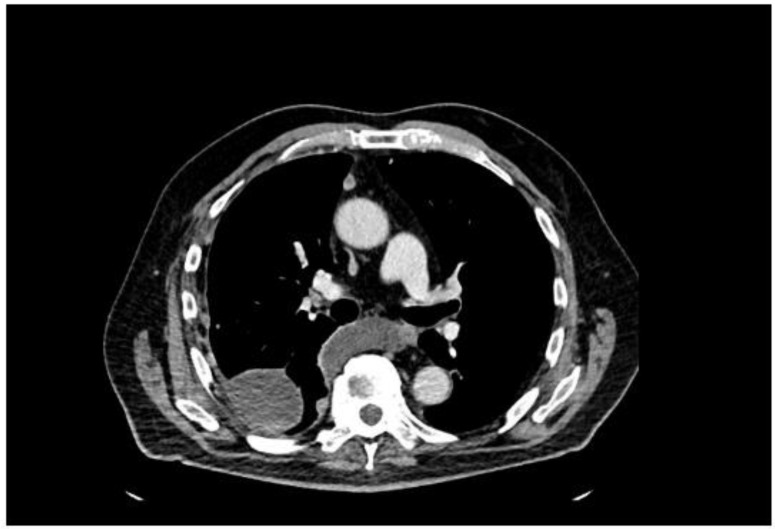
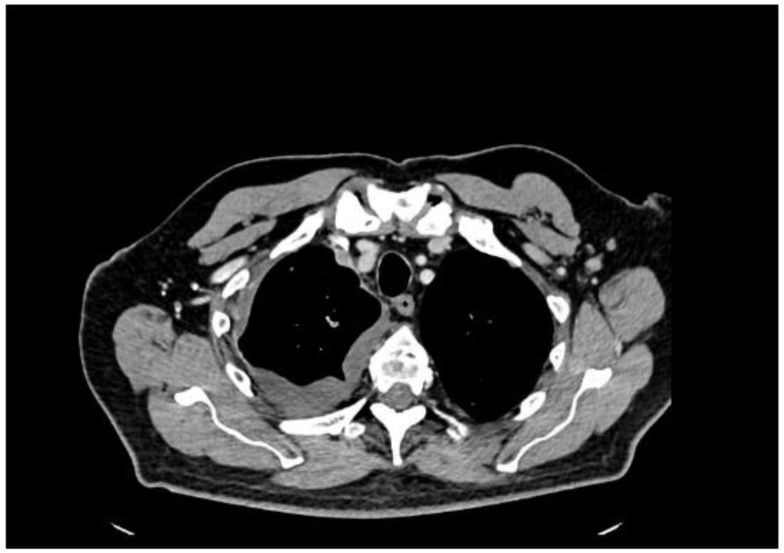
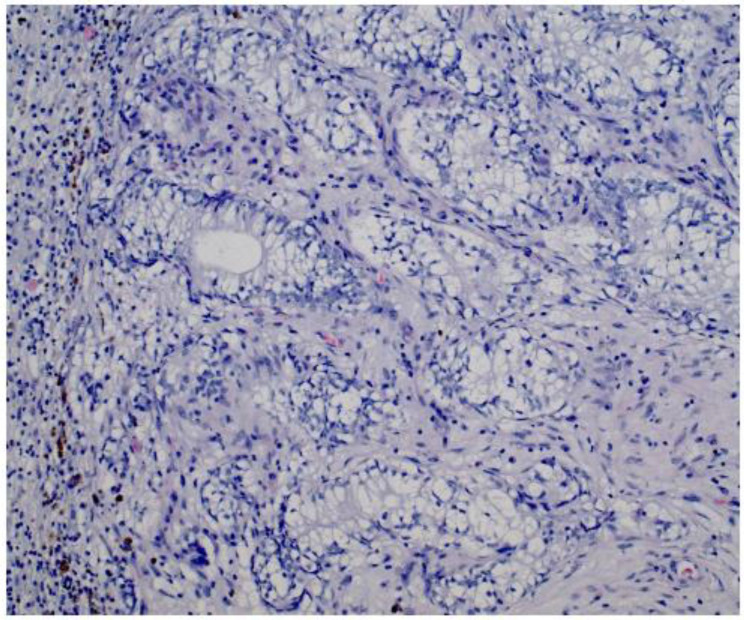
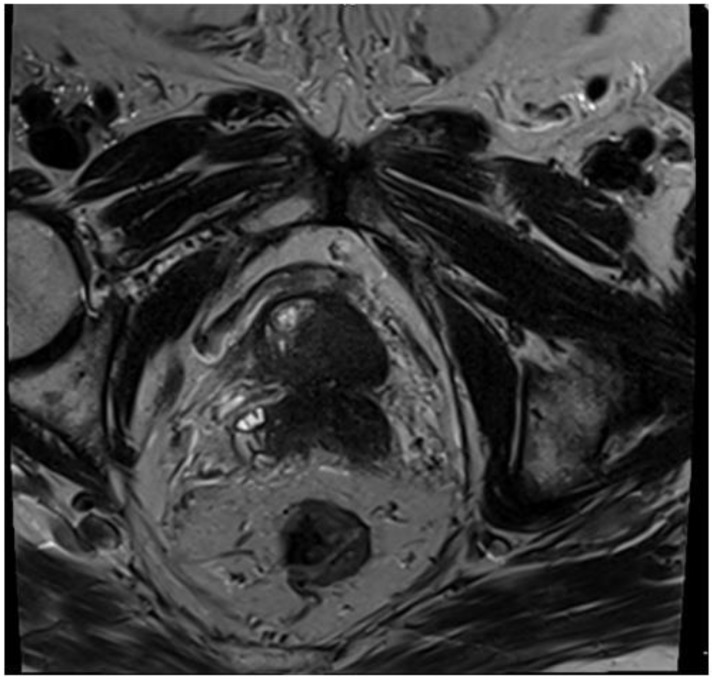
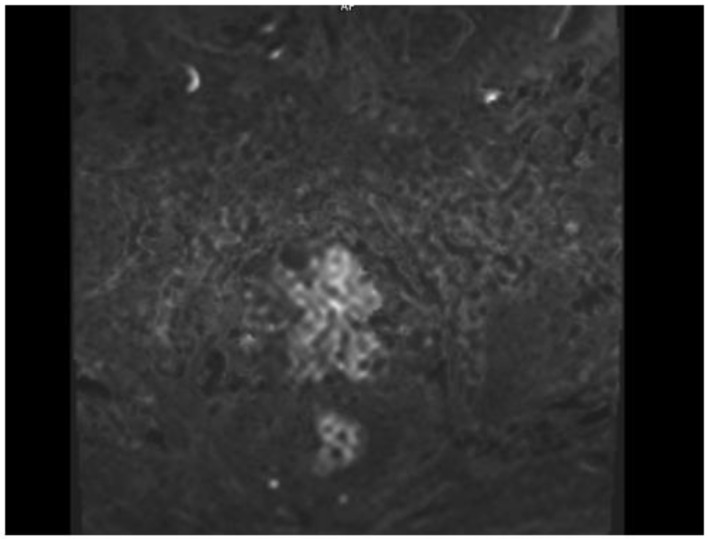
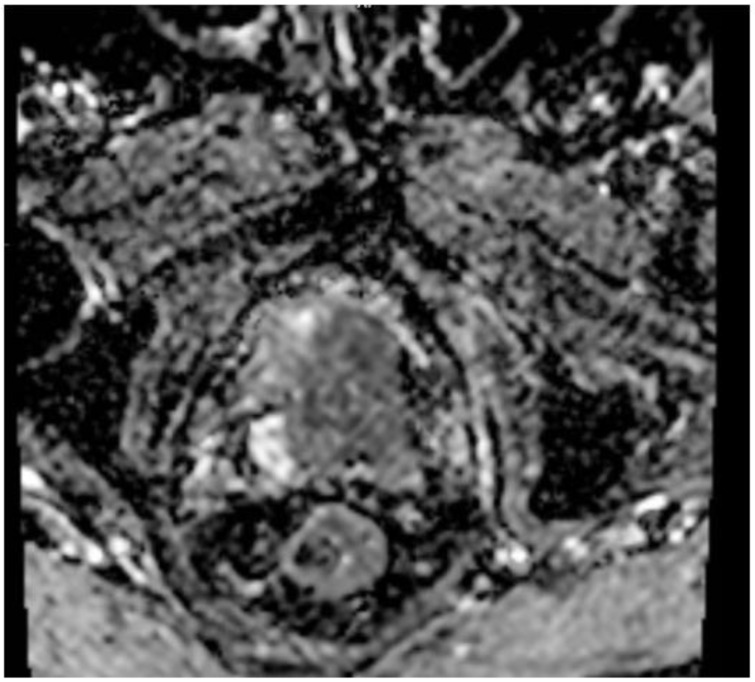
: Prostate cancer (PCa) is among the most commonly diagnosed malignancies in men worldwide. While bone and lymph nodes are the most frequent metastatic sites, prostate cancer cells have the potential to spread to virtually any organ, including the pleura, which is an exceedingly rare initial site of presentation that can mimic mesothelioma or primary lung cancer. : We describe a 77-year-old man who presented with exertional dyspnea and intermittent cough, initially suggesting a cardiopulmonary etiology. Imaging revealed multiple pleural nodules and an extensive right-sided pleural effusion. Despite a borderline serum prostate-specific antigen (PSA) level of 2.91 ng/mL, histopathology and immunohistochemistry of pleural biopsies confirmed metastatic prostate adenocarcinoma. Subsequent imaging identified a PIRADS 5 lesion in the prostate, and a biopsy confirmed ISUP Grade Group 5 disease (Gleason score 4 + 5 = 9). A bone scan showed no skeletal metastases, and a contrast-enhanced CT of the abdomen found no additional metastatic lesions. The patient was started on androgen deprivation therapy followed by abiraterone. This case underscores the diagnostic challenge posed by atypical metastatic presentations of prostate cancer. Low or moderately elevated PSA can obscure suspicion of prostate origin, especially with pleural-based lesions suggestive of mesothelioma. Immunohistochemical markers, including androgen receptors, AMACR, and Prostein, are critical for accurate diagnosis. : Clinicians must maintain a high index of suspicion for prostate cancer in older men with unexplained pleural effusions, nodules, or masses, even with low-normal PSA levels. Early recognition and prompt treatment can improve outcomes, despite the rarity and aggressiveness of pleural metastases.
前列腺癌(PCa)是全球男性中最常被诊断出的恶性肿瘤之一。虽然骨骼和淋巴结是最常见的转移部位,但前列腺癌细胞实际上有可能扩散到任何器官,包括胸膜,而胸膜是一个极其罕见的初始表现部位,可能会被误诊为间皮瘤或原发性肺癌。
我们描述了一名77岁男性,他出现劳力性呼吸困难和间歇性咳嗽,最初提示心肺病因。影像学检查发现多个胸膜结节和广泛的右侧胸腔积液。尽管血清前列腺特异性抗原(PSA)水平临界为2.91 ng/mL,但胸膜活检的组织病理学和免疫组化结果证实为转移性前列腺腺癌。随后的影像学检查在前列腺中发现了一个PI-RADS 5类病变,活检证实为ISUP 5级组疾病(Gleason评分4 + 5 = 9)。骨扫描显示无骨转移,腹部增强CT未发现其他转移病灶。患者开始接受雄激素剥夺治疗,随后使用阿比特龙。该病例强调了前列腺癌非典型转移表现所带来的诊断挑战。低或中度升高的PSA可能会掩盖对前列腺起源的怀疑,尤其是对于提示间皮瘤的胸膜病变。包括雄激素受体、AMACR和Prostein在内的免疫组化标志物对于准确诊断至关重要。
临床医生必须对有不明原因胸腔积液、结节或肿块的老年男性保持高度的前列腺癌怀疑指数,即使PSA水平处于正常低限。尽管胸膜转移罕见且具有侵袭性,但早期识别和及时治疗可改善预后。