Cheng Quankai, Zhou Sheng, Zhong Haicheng, Wang Ziming, Liu Chang, Sun Jingjing, Deng Jie
Department of Cardiology, The Second Affiliated Hospital of Xi'an Jiaotong University, Xi'an, Shaanxi, China.
Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Xi'an Jiaotong University, Xi'an, Shaanxi, China.
Front Public Health. 2025 Apr 25;13:1563631. doi: 10.3389/fpubh.2025.1563631. eCollection 2025.
With a rapidly growing and aging world population, ischemic heart disease (IHD) remains a major burden. This study aimed to reassess the prevalence trend of IHD from 1990 to 2021 from multiple dimensions to improve the shortcomings of the existing studies and provide a solid scientific basis for policymakers.
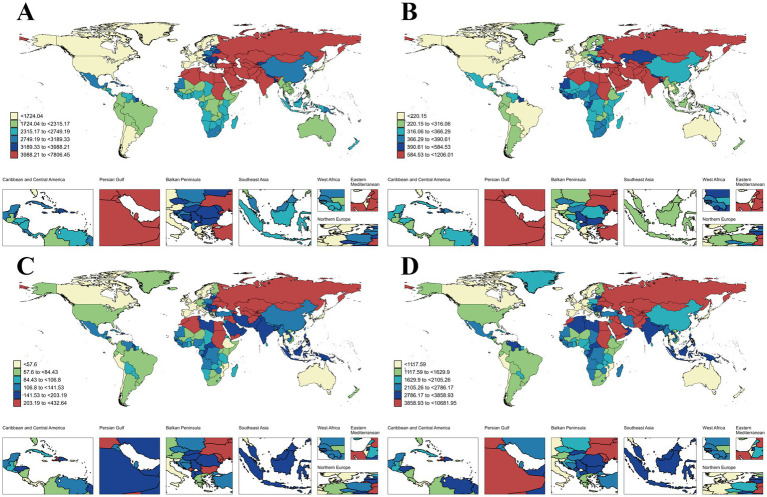
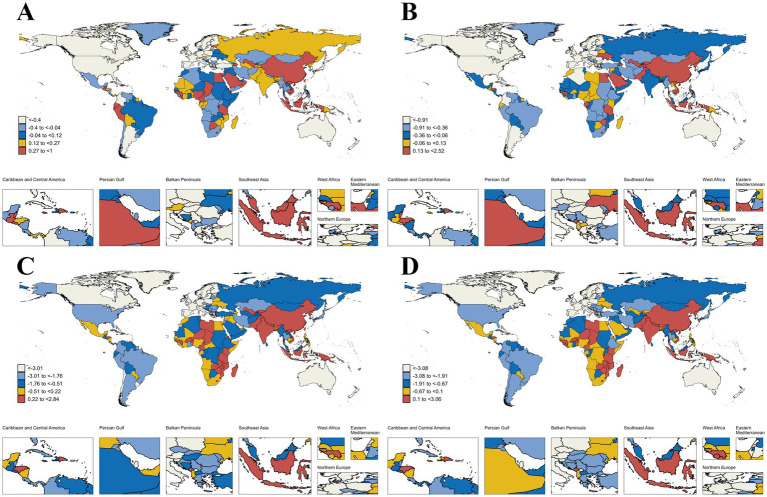
This study extracted data on the prevalence, incidence, mortality, disability-adjusted life years (DALYs), and associated risk factors of IHD from the global burden of disease (GBD) 2021 study. Descriptive, decomposition, and risk factor analyses were used to provide insights into the epidemiologic patterns of IHD from 1990 to 2021 and project the burden of IHD from 2022 to 2045. Potential differences in burden and risk factors based on age, sex, 21 GBD geographic regions, five social development index (SDI) regions, and 204 countries are highlighted.
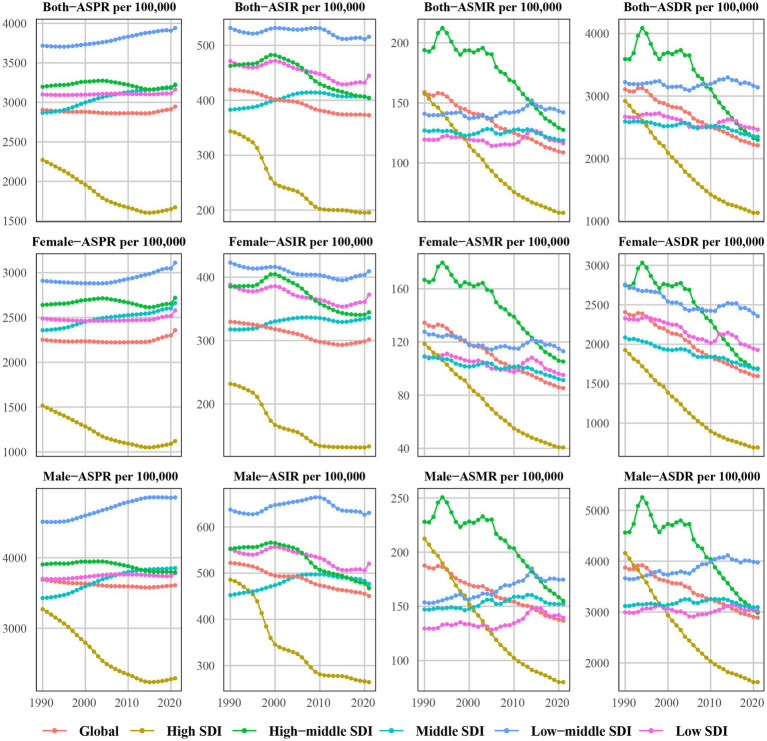
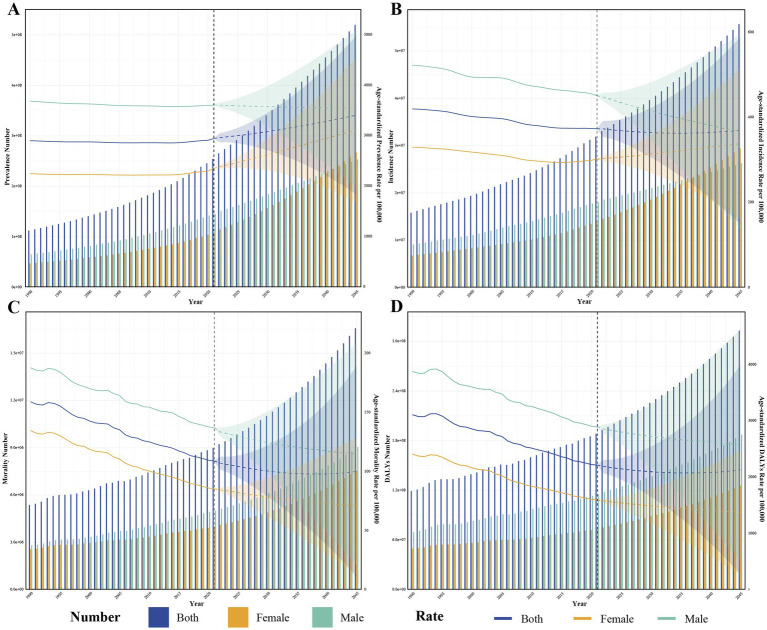
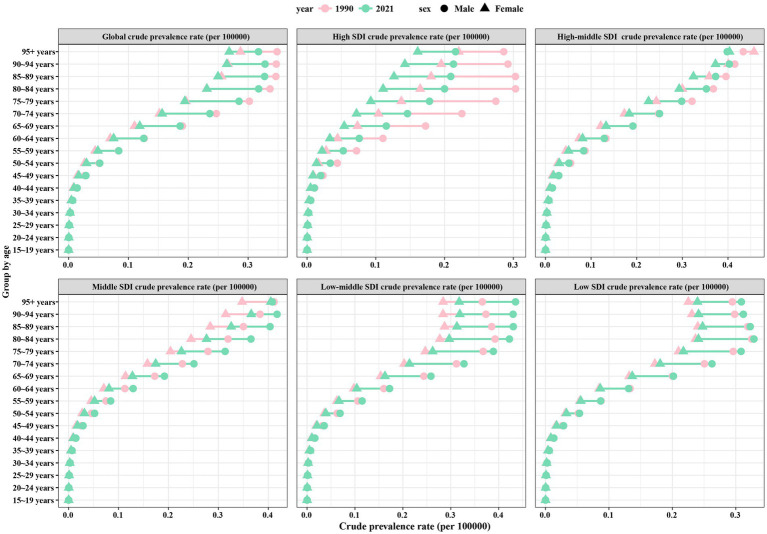
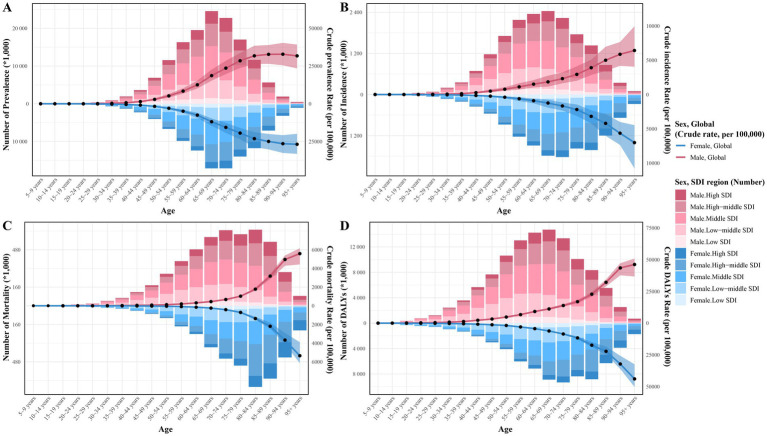
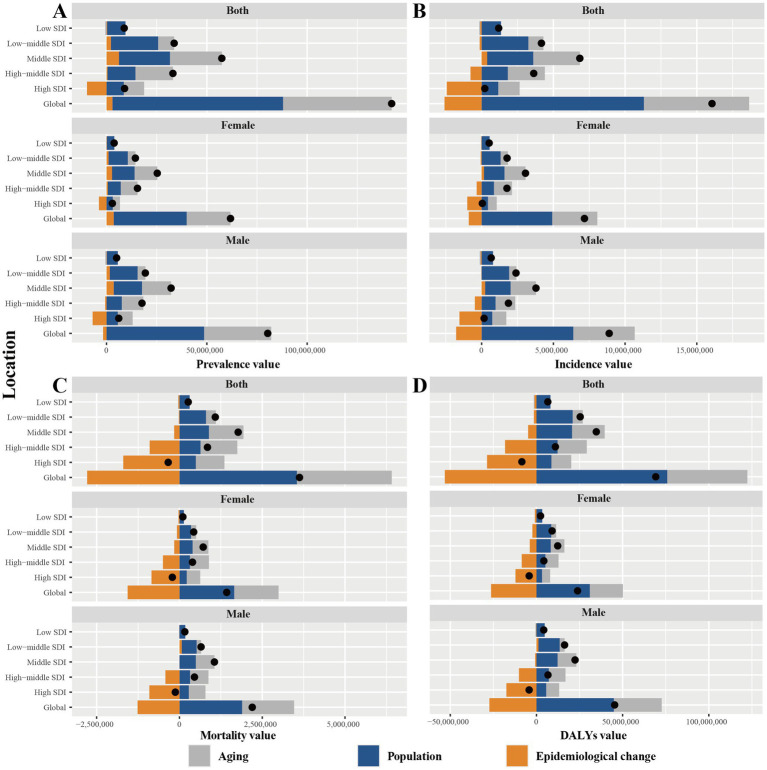
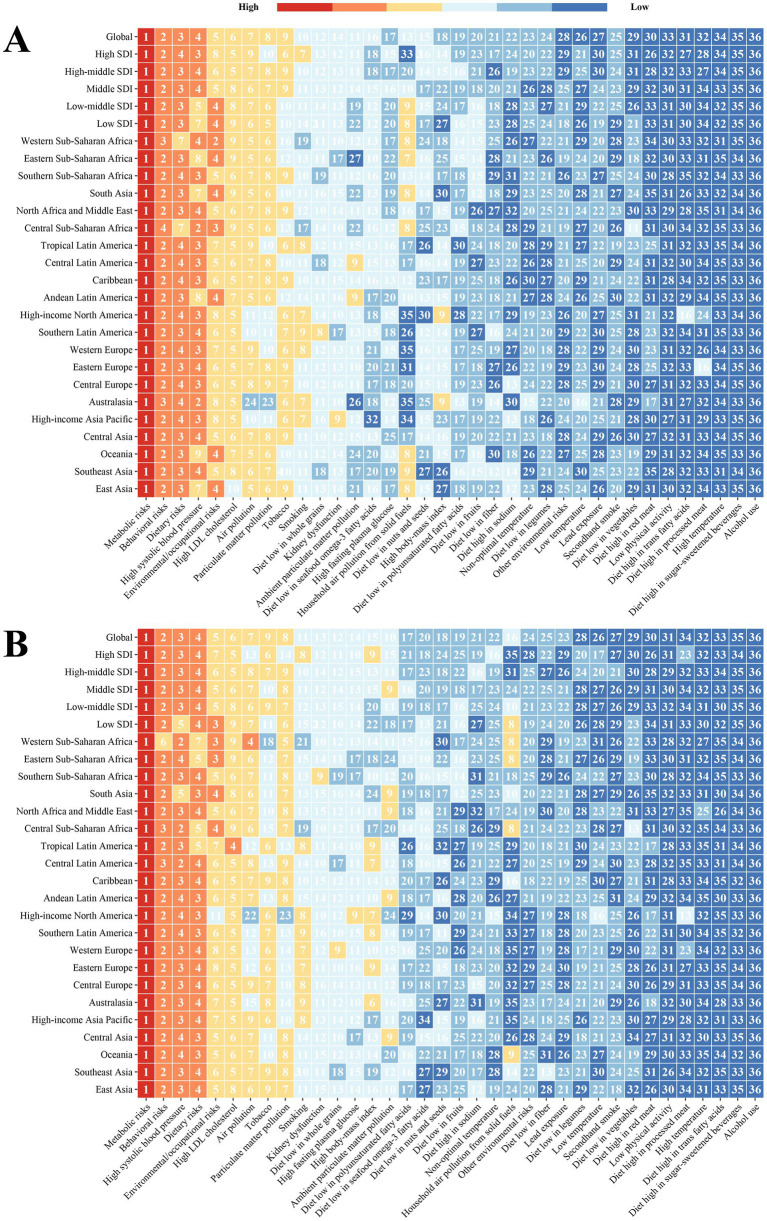
Globally, the age-standardized prevalence rate (ASPR) of IHD is increasing, while the age-standardized incidence rate (ASIR), age-standardized mortality rate (ASMR), and age-standardized disability-adjusted life years (ASDR) are decreasing. ASPR, ASIR, ASMR, and ASDR were highest in the low-middle SDI regions and lowest in the high SDI regions. ASMR and ASDR were highest in Nauru and lowest in Portugal. Men had an overall heavier burden of IHD than women; the 65-69 age group had the largest burden, and those aged >95 years had the highest crude incidence rate. In addition, the burden of IHD was negatively correlated with SDI across regions and countries, while decomposition analyses suggest that the main reasons for the current increase in the burden of IHD are aging and population growth. Risk factors have changed relatively little over the 32 years, with metabolic risk still ranking first. We forecast that the absolute burden of IHD will continue to increase till 2045; however, ASIR, ASMR, and ASDR will gradually decline.
From 1990 to 2021, the global burden of IHD generally increased and varied across regions, sex, and age groups. Due to increasing population growth and aging, there is an urgent need for strategically directed measures to reduce the burden of IHD.
随着世界人口的快速增长和老龄化,缺血性心脏病(IHD)仍然是一个主要负担。本研究旨在从多个维度重新评估1990年至2021年IHD的患病率趋势,以改进现有研究的不足,并为政策制定者提供坚实的科学依据。
本研究从《2021年全球疾病负担(GBD)研究》中提取了IHD的患病率、发病率、死亡率、伤残调整生命年(DALY)及相关危险因素的数据。采用描述性、分解性和危险因素分析,以深入了解1990年至2021年IHD的流行病学模式,并预测2022年至2045年IHD的负担。突出了基于年龄、性别、21个GBD地理区域、五个社会发展指数(SDI)区域和204个国家的负担和危险因素的潜在差异。
在全球范围内,IHD的年龄标准化患病率(ASPR)在上升,而年龄标准化发病率(ASIR)、年龄标准化死亡率(ASMR)和年龄标准化伤残调整生命年(ASDR)在下降。ASPR、ASIR、ASMR和ASDR在低中SDI区域最高,在高SDI区域最低。ASMR和ASDR在瑙鲁最高,在葡萄牙最低。男性IHD的总体负担比女性重;65 - 69岁年龄组的负担最大,95岁以上人群的粗发病率最高。此外,IHD的负担在各区域和国家与SDI呈负相关,而分解分析表明,目前IHD负担增加的主要原因是老龄化和人口增长。在这32年中,危险因素变化相对较小,代谢危险因素仍居首位。我们预测,IHD的绝对负担将持续增加至2045年;然而,ASIR、ASMR和ASDR将逐渐下降。
从1990年到2021年,全球IHD负担总体增加,且因区域、性别和年龄组而异。由于人口增长和老龄化加剧,迫切需要采取针对性的战略措施来减轻IHD负担。