Iyaniwura Sarafa A, Han Qing, Yong Ngem Bede, Rutayisire Ghislain, Adom-Konadu Agnes, Mbah Okwen Patrick, Tchouassi David Poumo, Badu Kingsley, Kong Jude Dzevela
Theoretical Biology and Biophysics, Theoretical Division, Los Alamos National Laboratory, Los Alamos, NM 87545, USA.
Laboratory for Industrial and Applied Mathematics (LIAM), Department of Mathematics and Statistics, York University, Toronto, M3J 1P3, Ontario, Canada.
Infect Dis Model. 2025 May 30;10(4):1103-1115. doi: 10.1016/j.idm.2025.05.006. eCollection 2025 Dec.
Despite significant global effort to control and eradicate malaria, many cases and deaths are still reported yearly. These efforts are hindered by several factors, including the severe underestimation of cases and deaths, especially in Africa.
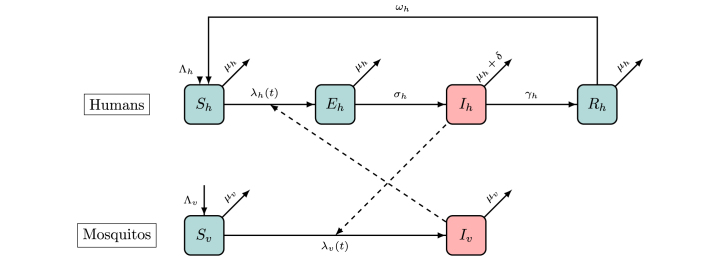
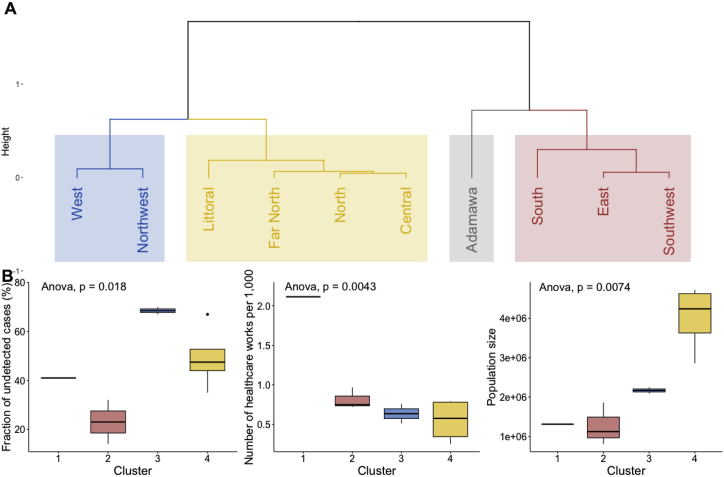
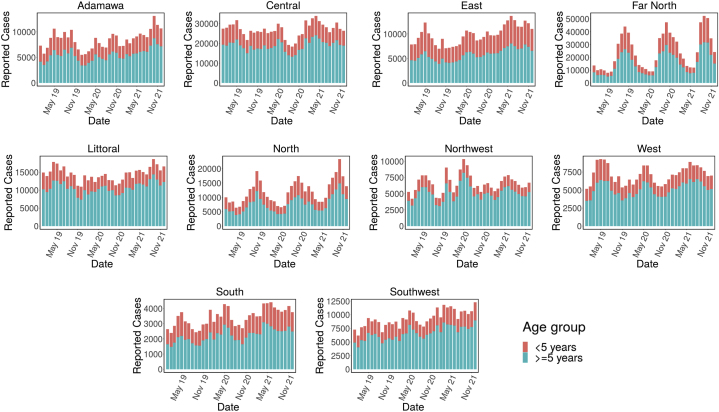
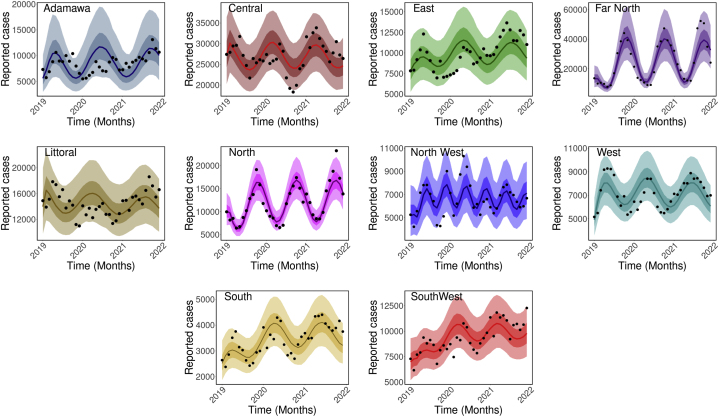
We used a mathematical model, incorporating the underestimation of cases and seasonality in mosquito biting rate, to study the malaria dynamics in Cameroon. Using a Bayesian inference framework, we calibrated our model to the monthly reported malaria cases in ten regions of Cameroon from 2019 to 2021 to quantify the underestimation of cases and estimate other important epidemiological parameters. We performed Hierarchical Clustering on Principal Components analysis to understand regional disparities, looking at underestimation rates, population sizes, healthcare personnel, and healthcare facilities per 1000 people.
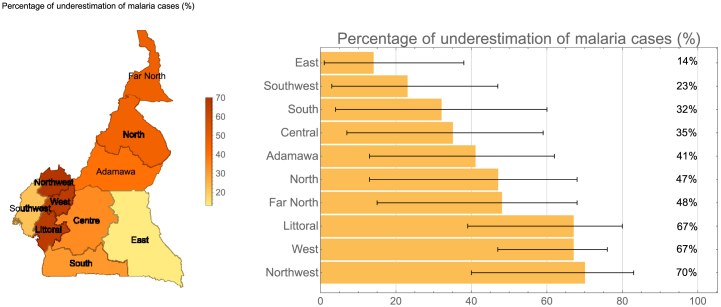
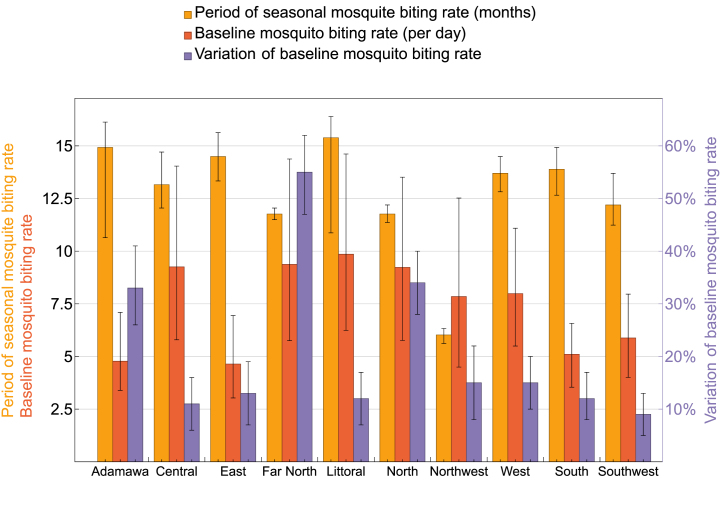
We found varying levels of case underestimation across regions, with the East region having the lowest (14 %) and the Northwest having the highest (70 %). The mosquito biting rate peaks once every year in most regions, except in the Northwest where it peaks every 6.02 months and in Littoral every 15 months. We estimated a median mosquito biting rate of over 5 bites/day for most regions with Littoral having the highest (9.86 bites/day). Two regions have rates below five: Adamawa (4.78 bites/day) and East (4.64 bites/day).
The low case estimation underscores the pressing requirement to bolster reporting and surveillance systems. Regions in Cameroon display a range of unique features contributing to the differing levels of underestimation. These distinctions should be considered when evaluating the efficacy of community-based interventions.
尽管全球为控制和消除疟疾付出了巨大努力,但每年仍有许多病例报告和死亡。这些努力受到多种因素的阻碍,包括对病例和死亡的严重低估,尤其是在非洲。
我们使用了一个数学模型,该模型纳入了病例低估和蚊虫叮咬率的季节性因素,以研究喀麦隆的疟疾动态。我们使用贝叶斯推理框架,将模型校准到喀麦隆十个地区2019年至2021年每月报告的疟疾病例,以量化病例的低估情况并估计其他重要的流行病学参数。我们对主成分分析进行层次聚类,以了解区域差异,观察每千人的低估率、人口规模、医护人员和医疗设施情况。
我们发现各地区病例低估程度各不相同,东部地区最低(14%),西北部最高(70%)。除西北部每6.02个月出现一次高峰、滨海区每15个月出现一次高峰外,大多数地区蚊虫叮咬率每年出现一次高峰。我们估计大多数地区蚊虫叮咬率中位数超过每天5次,滨海区最高(每天9.86次)。有两个地区低于5次:阿达马瓦(每天4.78次)和东部(每天4.64次)。
病例估计数低凸显了加强报告和监测系统的迫切需求。喀麦隆各地区呈现出一系列独特特征,导致了不同程度的低估。在评估基于社区的干预措施的效果时,应考虑这些差异。