Lawson Nikki R, Achuff Barbara Jo, Ankola Ashish, Guffey Danielle, Lopez Keila, Afonso Natasha
Department of Pediatrics, Division of Critical Care Medicine, Baylor College of Medicine, Houston, TX, United States.
Department of Pediatrics, Division of Critical Care Medicine, Vanderbilt University Medical Center, Nashville, TN, United States.
Front Pediatr. 2025 Jul 16;13:1577461. doi: 10.3389/fped.2025.1577461. eCollection 2025.
Disparities in congenital heart disease, pediatric intensive care unit (ICU) outcomes, and acute pain control are common. The impact of patient race, ethnicity, and language on postoperative sedation and analgesia for pediatric patients undergoing cardiac surgery is unknown.
This study aims to investigate whether there are differences in sedation and analgesia in patients undergoing cardiac surgery according to patient race, ethnicity, and language in a study site that uses protocolized postoperative sedation and analgesia. We hypothesized that non-white and patients who prefer a language other than English would have differences in total doses of sedation compared with their white and English-speaking counterparts.
This is a single-center, retrospective, observational cohort of pediatric patients admitted postoperatively to the cardiac ICU.
The study took place in an urban, quaternary, academic pediatric referral center.
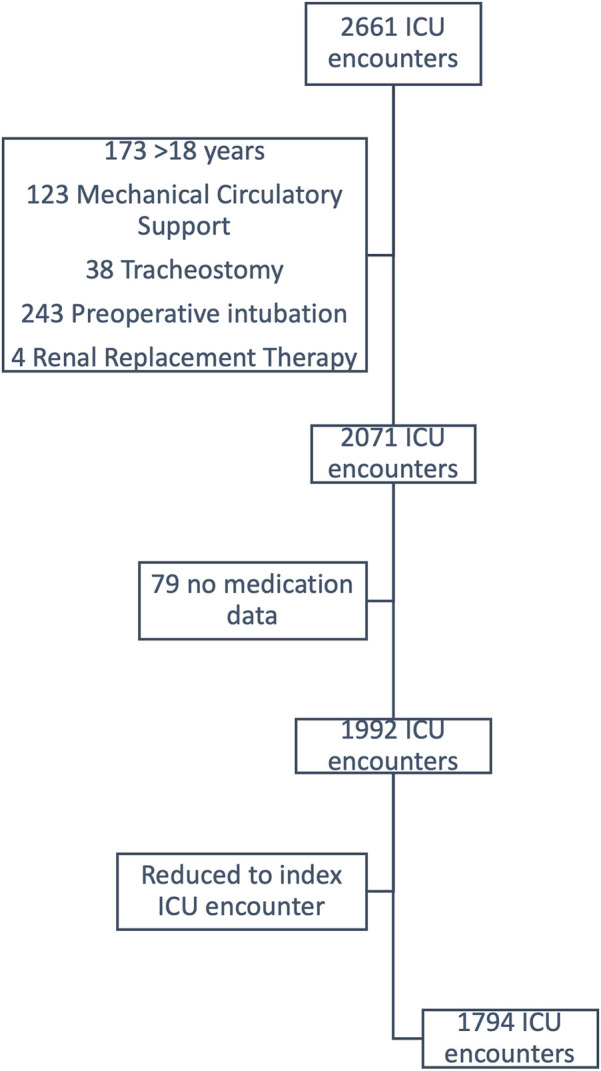
All pediatric patients, age 0-18 years, admitted to the cardiac ICU following their index cardiac surgery from 7/1/2018 to 6/30/2022 were included. Patients requiring renal replacement therapy, non-cardiac surgery during the same admission, tracheostomy, preoperative mechanical ventilation, or mechanical circulatory support prior to or following cardiac surgery were excluded.
Exposure variables included patient race and ethnicity, preferred language, age, gender, Society of Thoracic Surgeons-European Association for Cardiothoracic Surgery category, use of cardiopulmonary bypass, duration of postoperative mechanical ventilation, and delayed sternal closure (DSC).
The primary outcome was weight-adjusted doses of opioids in morphine equivalents, benzodiazepines in midazolam equivalents, and dexmedetomidine received in the first 72 h postoperatively.
There were 1,794 postoperative admissions. 100% of patients received opioids, 42.5% received benzodiazepines, and 85% received dexmedetomidine. There were no differences in opioid, benzodiazepine, or dexmedetomidine doses according to patient race and ethnicity or preferred language. Patient race, ethnicity, and language were not associated with opioid or benzodiazepine dose in multivariable quantile regression. Multivariable regression for dexmedetomidine demonstrated similar results with age also being inversely correlated.
and Relevance: Doses of postoperative sedation and analgesia are not correlated with patient race, ethnicity, and language. Factors that were associated with differences in medication doses are reflective of postoperative acuity and are expected. Protocolized sedation and analgesia may be responsible for the lack of differences seen in this study when compared with other studies in similar settings. Future studies should compare protocolized and non-protocolized sedation and analgesia to further evaluate the protective effects of protocols against bias in clinical settings.
先天性心脏病、儿科重症监护病房(ICU)治疗结果以及急性疼痛控制方面的差异很常见。患者种族、族裔和语言对接受心脏手术的儿科患者术后镇静和镇痛的影响尚不清楚。
本研究旨在调查在一个采用标准化术后镇静和镇痛方案的研究地点,接受心脏手术的患者在镇静和镇痛方面是否因患者种族、族裔和语言而存在差异。我们假设,与白人及说英语的患者相比,非白人患者以及更喜欢使用英语以外语言的患者在镇静总剂量方面会存在差异。
这是一项针对术后入住心脏ICU的儿科患者的单中心回顾性观察队列研究。
该研究在一家城市四级学术儿科转诊中心进行。
纳入了2018年7月1日至2022年6月30日期间接受首次心脏手术后入住心脏ICU的所有0至18岁儿科患者。排除了需要肾脏替代治疗、在同一住院期间进行非心脏手术、气管切开术、术前机械通气或心脏手术前后需要机械循环支持的患者。
暴露变量包括患者种族和族裔、首选语言、年龄、性别、胸外科医师协会 - 欧洲心胸外科协会分类、体外循环的使用、术后机械通气持续时间以及延迟胸骨闭合(DSC)。
主要结局是术后前72小时按体重调整的吗啡当量的阿片类药物剂量、咪达唑仑当量的苯二氮䓬类药物剂量以及右美托咪定的剂量。
共有1794例术后入院患者。100%的患者接受了阿片类药物,42.5%的患者接受了苯二氮䓬类药物,85%的患者接受了右美托咪定。根据患者种族、族裔或首选语言,阿片类药物、苯二氮䓬类药物或右美托咪定的剂量没有差异。在多变量分位数回归中,患者种族、族裔和语言与阿片类药物或苯二氮䓬类药物剂量无关。右美托咪定的多变量回归显示了类似的结果,年龄也呈负相关。
术后镇静和镇痛剂量与患者种族、族裔和语言无关。与药物剂量差异相关的因素反映了术后的严重程度,这是预期的。与类似环境下的其他研究相比,标准化镇静和镇痛可能是本研究中未观察到差异的原因。未来的研究应比较标准化和非标准化的镇静和镇痛,以进一步评估方案在临床环境中对抗偏倚的保护作用。