Shen Peter, Swaroop Vineeta T, Rojas Ana Marie, Hirsch Josephine, Chu David I, Papadakis Jaclyn L, Bowman Robin, Larson Jill E
Northwestern University Feinberg School of Medicine, Chicago, IL, USA.
Ann and Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, USA.
J Pediatr Soc North Am. 2025 Jun 9;12:100205. doi: 10.1016/j.jposna.2025.100205. eCollection 2025 Aug.
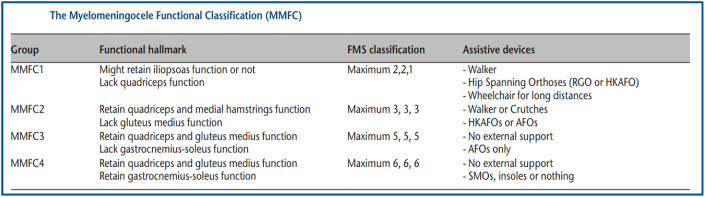
The Myelomeningocele Functional Classification (MMFC) provides a comprehensive summary of functional mobility in patients with spina bifida (SB). The hallmark of MMFC1 patients is the deficiency of gravity-dependent quadriceps musculature strength which precludes independent ambulation but not supportive standing. Limited data exist on the clinical value of supportive standing in this population. The purpose of this study was to identify orthopaedic outcomes and patient-reported quality of life (QOL) scores in MMFC1 spina bifida patients and investigate their relationship to continued supportive standing.
A retrospective chart review was performed between 2004 and 2023 of all patients with SB treated at a regional tertiary pediatric care center. Patients were excluded if manual muscle testing did not fit the criteria for MMFC1 classification. Demographic, clinical outcomes, and the Patient-Reported Outcomes Measurement Information System (PROMIS) scores were reviewed. Supportive standing history was extracted from chart review and analyzed relative to outcome measures. Statistical analyses were reported with < .05 reaching significance.
In total, 2,228 patients in our SB clinic were screened with 78 (3.5%) meeting the MMFC1 inclusion criteria. Thirty-three patients (42%) had at least one fracture with 25 (32%) of those patients having a femur fracture. Thirty-nine patients (50%) had at least one pressure sore with 23 (29%) of those patients having a sacral/ischial wound. Those who continued to stand at the most recent follow-up showed a statistically significant decrease in the number of skin wounds compared with those who discontinued standing, but no difference in number of fractures. A significant difference in the Neurogenic Bladder scores was noted in standing patients with higher bladder QOL scores.
MMFC1 patients with spina bifida are at risk for sustaining fractures and/or sacral/ischial pressure sores, but discontinuing supported standing is associated with an increased pressure wound risk. Additionally, patients who continued to stand had higher bladder QOL scores. Utilizing supportive standing in conjunction with multidisciplinary care may decrease the risk of fractures and pressure sores and improve QOL in MMFC1 patients with spina bifida.
(1)Myelomeningocele Functional Classification 1 (MMFC1) patients with spina bifida are at risk of incurring a femur fracture regardless of supportive standing.(2)MMFC1 spina bifida patients who continue to stand have significantly fewer number of pressure sores.(3)Improved neurogenic bladder quality of life scores were correlated with MMFC1 spina bifida patients who continued supportive standing.(4)A multidisciplinary team approach is needed to prevent barriers to care and improve quality of life in MMFC1 spina bifida patients.
Level III.
脊髓脊膜膨出功能分类(MMFC)全面总结了脊柱裂(SB)患者的功能活动能力。MMFC1级患者的典型特征是依赖重力的股四头肌肌力不足,这使得他们无法独立行走,但可以在支撑下站立。关于支撑站立在该人群中的临床价值的数据有限。本研究的目的是确定MMFC1级脊柱裂患者的骨科治疗结果和患者报告的生活质量(QOL)评分,并研究它们与持续支撑站立的关系。
对2004年至2023年期间在一家地区三级儿科护理中心接受治疗的所有脊柱裂患者进行回顾性病历审查。如果徒手肌力测试不符合MMFC1分类标准,则将患者排除。审查了人口统计学、临床结果以及患者报告结果测量信息系统(PROMIS)评分。从病历审查中提取支撑站立史,并相对于结果指标进行分析。统计分析报告时P <.05具有统计学意义。
在我们的脊柱裂诊所共筛查了2228例患者,其中78例(3.5%)符合MMFC1纳入标准。33例患者(42%)至少发生过一次骨折,其中25例(32%)为股骨骨折。39例患者(50%)至少有一处压疮,其中23例(29%)为骶骨/坐骨伤口。与停止站立的患者相比,在最近一次随访时仍继续站立的患者皮肤伤口数量在统计学上显著减少,但骨折数量没有差异。在站立的患者中,神经源性膀胱评分存在显著差异,站立患者的膀胱生活质量得分更高。
MMFC1级脊柱裂患者有发生骨折和/或骶骨/坐骨压疮的风险,但停止支撑站立与压疮风险增加有关。此外,继续站立的患者膀胱生活质量得分更高。将支撑站立与多学科护理相结合,可能会降低MMFC1级脊柱裂患者骨折和压疮的风险,并改善其生活质量。
(1)MMFC1级脊柱裂患者无论是否有支撑站立都有发生股骨骨折的风险。(2)继续站立的MMFC1级脊柱裂患者压疮数量明显较少。(3)神经源性膀胱生活质量得分的提高与继续支撑站立的MMFC1级脊柱裂患者相关。(4)需要采用多学科团队方法来预防护理障碍并改善MMFC1级脊柱裂患者的生活质量。
三级。