Garrett J, Fenwick J M, Taylor G, Mitchell E, Stewart J, Rea H
Department of Respiratory Medicine, Green Lane Hospital, Auckland, New Zealand.
Thorax. 1994 Oct;49(10):976-83. doi: 10.1136/thx.49.10.976.
Previous work has indicated a high rate of non-attendance at hospital based clinics among young, multiracial asthmatic patients of lower socioeconomic class. The efficacy of delivering asthma education from a community health centre established in a multiracial working class neighbourhood was evaluated.
A prospective controlled study was performed in which asthmatic subjects aged between two and 55 years attending a hospital emergency room with acute asthma and living within a defined geographical area of high emergency room users were randomised to the usual follow up or the education centre plus usual follow up. Measurements were taken at entry into the study and again nine months later.
At nine months patients randomised to the education centre had more preventive medications, more peak expiratory flow meters and better flow meter technique, more self-management plans, better knowledge of appropriate action to take when confronted with worsening asthma, less nocturnal awakening, and better self-reported asthma control than the control group. There was no difference between the study groups in measurements of compliance, hospital admission, days lost from school or work, or emergency room use.
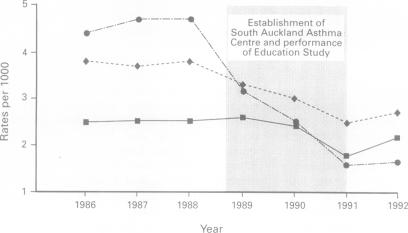
The main effects of education were on asthma knowledge and self-management skills, whilst improvements in asthma morbidity were small. Potential reasons for this include heterogeneous study population (in terms of baseline self-management skills, asthma severity, ethnicity and age), pragmatic study design, insensitivity of many of the measurements of morbidity, the modest effectiveness of a single time limited education programme, and inability to limit the effects of such a large community based study to the intervention group (there was a 67% reduction in asthma admissions during the study period from the geographical area targeted compared with a 22% reduction for the rest of Auckland).
此前的研究表明,社会经济地位较低的年轻多族裔哮喘患者在医院门诊的就诊率较低。本研究评估了在一个多族裔工人阶级社区设立的社区健康中心开展哮喘教育的效果。
进行了一项前瞻性对照研究,将年龄在2至55岁之间、因急性哮喘到医院急诊室就诊且居住在急诊室高使用率特定地理区域内的哮喘患者随机分为常规随访组或教育中心加常规随访组。在研究开始时和九个月后再次进行测量。
九个月时,随机分配到教育中心的患者比对照组有更多的预防性药物、更多的呼气峰值流速仪且流速仪使用技术更好、更多的自我管理计划、在哮喘恶化时采取适当行动的知识更丰富、夜间觉醒更少,且自我报告的哮喘控制情况更好。两组在依从性、住院率、缺课或旷工天数或急诊室就诊次数的测量上没有差异。
教育的主要效果体现在哮喘知识和自我管理技能方面,而哮喘发病率的改善较小。其潜在原因包括研究人群的异质性(在基线自我管理技能、哮喘严重程度、种族和年龄方面)、务实的研究设计、许多发病率测量方法不敏感、单次限时教育计划的效果有限,以及无法将如此大规模的社区研究的效果局限于干预组(与奥克兰其他地区22%的下降相比,研究期间目标地理区域的哮喘住院率下降了67%)。