Lim K L, Abdul-Wahab R, Lowe J, Powell R J
Department of Immunology, University Hospital, Queens Medical Centre, Nottingham, United Kingdom.
Ann Rheum Dis. 1994 Mar;53(3):178-82. doi: 10.1136/ard.53.3.178.
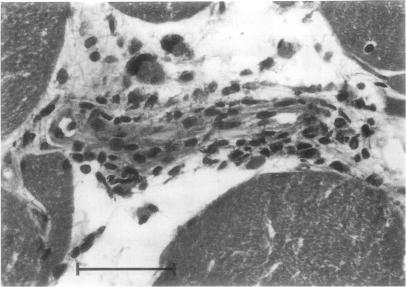
To investigate the incidence and significance of Type II fibre atrophy, vessel wall thickening, lymphocytic vasculitis and myositis in needle quadriceps muscle biopsies from patients with systemic lupus erythematosus (SLE) and their correlations with clinical and laboratory parameters.
Needle quadriceps muscle biopsies from 55 patients with SLE and 26 controls were prospectively examined. Clinical and laboratory parameters recorded at the time of muscle biopsy included arthralgia, arthritis, myalgia, proximal weakness, vasculitic rashes, Schirmer test, ENA antibodies, ESR, serum creatine kinase (CK) and plasma C3 degradation products.
Abnormal muscle biopsies were significantly more frequent in patients with SLE compared with controls (P < 0.005). None of the controls had lymphocytic vasculitis and/or myositis. The difference in incidence between patients with SLE and controls for lymphocytic vasculitis was significant at P < 0.005. Due to the small number of SLE patients with myositis, the difference in incidence for this abnormal finding reached only P = 0.09. In the SLE patient group, lymphocytic vasculitis was associated with significantly higher ESR values (P = 0.007) and higher incidence of arthritis (P = 0.01); and appears to characterise a subset of patients with positive Schirmer tests, anti-Ro and/or anti-La antibodies. Raised serum CK was found to correspond with underlying myositis in patients with SLE and these patients also had an increased incidence of symptoms of proximal weakness and/or anti-RNP antibodies. In contrast, both Type II fibre atrophy and vessel wall thickening failed to correlate with any of the clinical and laboratory parameters studied and appear to be non-specific findings.
Abnormal muscle biopsies are common in patients with SLE and the presence of lymphocytic vasculitis and/or myositis signify pathology in these patients. Histopathological abnormalities in needle quadriceps muscle biopsies are further valuable parameters in the assessment of patients with SLE.
研究系统性红斑狼疮(SLE)患者股四头肌针吸活检中II型纤维萎缩、血管壁增厚、淋巴细胞性血管炎和肌炎的发生率及意义,以及它们与临床和实验室参数的相关性。
前瞻性检查了55例SLE患者和26例对照者的股四头肌针吸活检。肌肉活检时记录的临床和实验室参数包括关节痛、关节炎、肌痛、近端肌无力、血管炎性皮疹、Schirmer试验、可提取性核抗原(ENA)抗体、红细胞沉降率(ESR)、血清肌酸激酶(CK)和血浆C3降解产物。
与对照组相比,SLE患者肌肉活检异常更为常见(P<0.005)。对照组均无淋巴细胞性血管炎和/或肌炎。SLE患者与对照组淋巴细胞性血管炎的发生率差异有统计学意义,P<0.005。由于SLE肌炎患者数量较少,这一异常发现的发生率差异仅为P = 0.09。在SLE患者组中,淋巴细胞性血管炎与ESR值显著升高(P = 0.007)和关节炎发生率较高(P = 0.01)相关;似乎是Schirmer试验阳性、抗Ro和/或抗La抗体阳性患者亚组的特征。发现SLE患者血清CK升高与潜在的肌炎相关,这些患者近端肌无力症状和/或抗核糖核蛋白(RNP)抗体的发生率也增加。相比之下,II型纤维萎缩和血管壁增厚均与所研究的任何临床和实验室参数无关,似乎是非特异性发现。
SLE患者肌肉活检异常常见,淋巴细胞性血管炎和/或肌炎的存在表明这些患者存在病理改变。股四头肌针吸活检的组织病理学异常是评估SLE患者的进一步有价值的参数。