Anon Jack B, Jacobs Michael R, Poole Michael D, Ambrose Paul G, Benninger Mark S, Hadley James A, Craig William A
University of Pittsburgh, School of Medicine, USA.
Otolaryngol Head Neck Surg. 2004 Jan;130(1 Suppl):1-45. doi: 10.1016/j.otohns.2003.12.003.
Treatment guidelines developed by the Sinus and Allergy Health Partnership for acute bacterial rhinosinusitis (ABRS) were originally published in 2000. These guidelines were designed to: (1) educate clinicians and patients (or patients’ families) about the differences between viral and bacterial rhinosinusitis; (2) reduce the use of antibiotics for nonbacterial nasal/sinus disease; (3) provide recommendations for the diagnosis and optimal treatment of ABRS; (4) promote the use of appropriate antibiotic therapy when bacterial infection is likely; and (5) describe the current understanding of pharmacokinetic and pharmacodynamics and how they relate to the effectiveness of antimicrobial therapy. The original guidelines are updated here to include the most recent information on management principles, antimicrobial susceptibility patterns, and therapeutic options.
An estimated 20 million cases of ABRS occur annually in the United States. According to National Ambulatory Medical Care Survey (NAMCS) data, sinusitis is the fifth most common diagnosis for which an antibiotic is prescribed. Sinusitis accounted for 9% and 21% of all pediatric and adult antibiotic prescriptions, respectively, written in 2002. The primary diagnosis of sinusitis results in expenditures of approximately $3.5 billion per year in the United States.
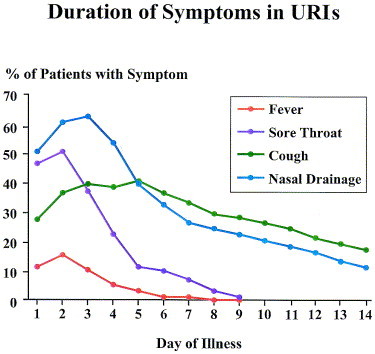
ABRS is most often preceded by a viral upper respiratory tract infection (URI). Allergy, trauma, dental infection, or other factors that lead to inflammation of the nose and paranasal sinuses may also predispose individuals to developing ABRS. Patients with a “common cold” (viral URI) usually report some combination of the following symptoms: sneezing, rhinorrhea, nasal congestion, hyposmia/anosmia, facial pressure, postnasal drip, sore throat, cough, ear fullness, fever, and myalgia. A change in the color or the characteristic of the nasal discharge is not a specific sign of a bacterial infection. Bacterial superinfection may occur at any time during the course of a viral URI. The risk that bacterial superinfection has occurred is greater if the illness is still present after 10 days. Because there may be cases that fall out of the “norm” of this typical progression, practicing clinicians need to rely on their clinical judgment when using these guidelines. In general, however, a diagnosis of ABRS may be made in adults or children with symptoms of a viral URI that have not improved after 10 days or worsen after 5 to 7 days. There may be some or all of the following signs and symptoms: nasal drainage, nasal congestion, facial pressure/pain (especially when unilateral and focused in the region of a particular sinus), postnasal drainage, hyposmia/anosmia, fever, cough, fatigue, maxillary dental pain, and ear pressure/fullness. Physical examination provides limited information in the diagnosis of ABRS. While sometimes helpful, plain film radiographs, computed tomography (CT), and magnetic resonance imaging scans are not necessary for cases of ABRS.
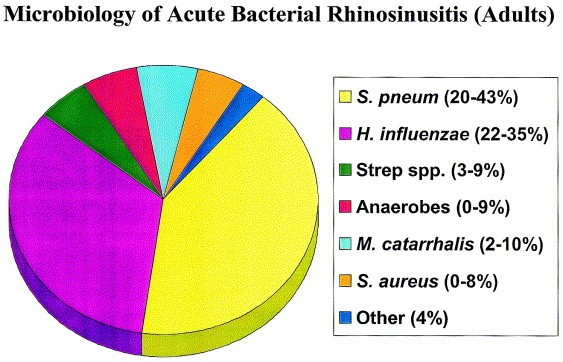
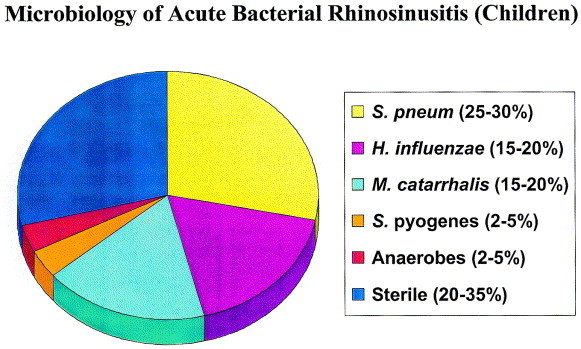
The most common bacterial species isolated from the maxillary sinuses of patients with ABRS are , , and , the latter being more common in children. Other streptococcal species, anaerobic bacteria and cause a small percentage of cases.
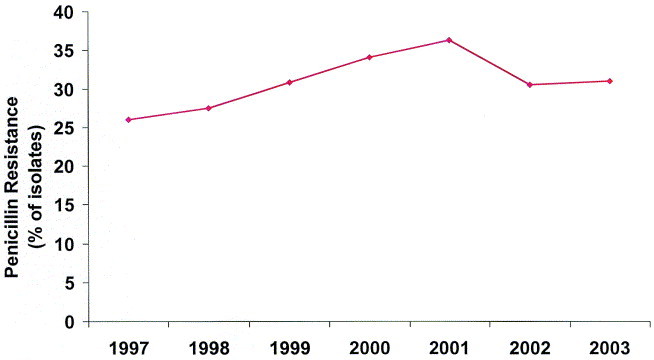
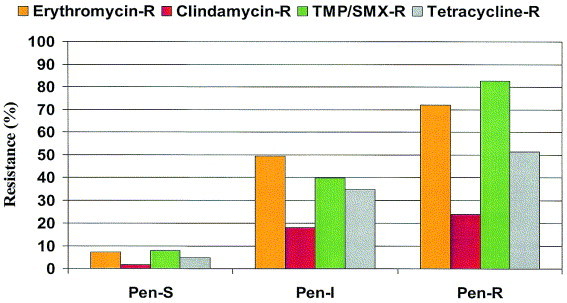
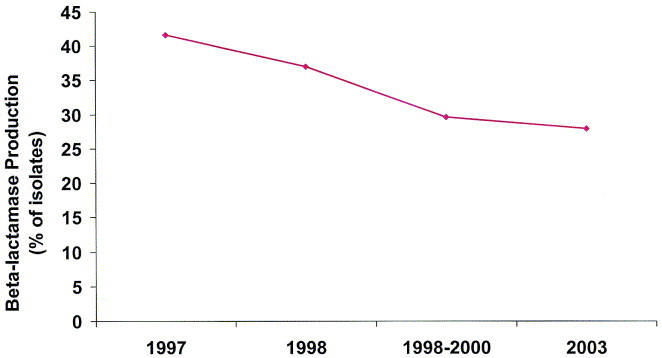
The increasing prevalence of penicillin nonsusceptibility and resistance to other drug classes among has been a problem in the United States, with 15% being penicillin-intermediate and 25% being penicillin-resistant in recent studies. Resistance to macrolides and trimethoprim/sulfamethoxazole (TMP/SMX) is also common in . The prevalence of β-lactamase-producing isolates of is approximately 30%, while essentially all isolates produce β-lactamases. Resistance of to TMP/SMX is also common.
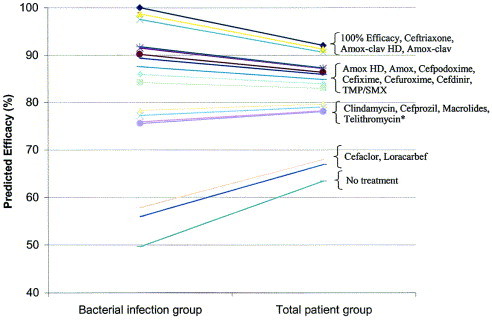
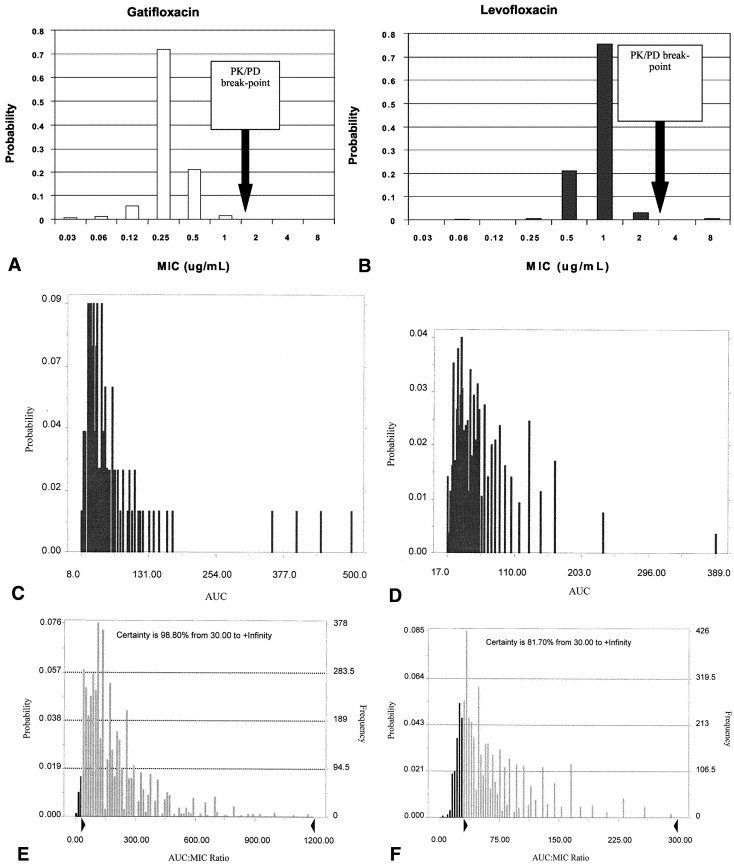
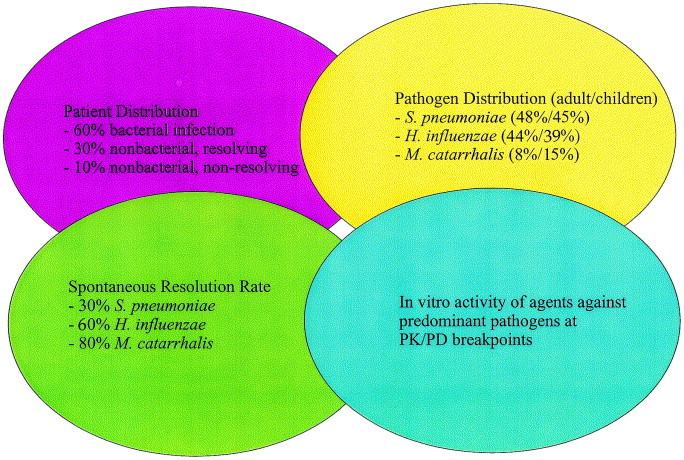
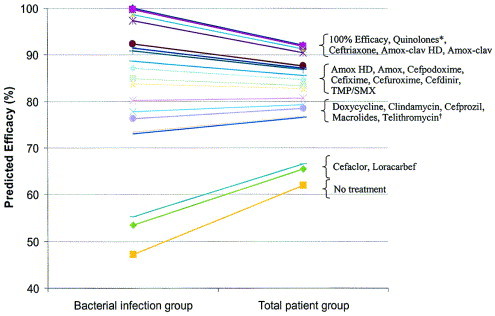
These guidelines apply to both adults and children. When selecting antibiotic therapy for ABRS, the clinician should consider the severity of the disease, the rate of progression of the disease, and recent antibiotic exposure. The guidelines now divide patients with ABRS into two general categories: (1) those with mild symptoms who have not received antibiotics within the past 4 to 6 weeks, and (2) those with mild disease who have received antibiotics within the past 4 to 6 weeks or those with moderate disease regardless of recent antibiotic exposure. The difference in severity of disease does not imply infection with a resistant pathogen. Rather, this terminology indicates the relative degree of acceptance of possible treatment failure and the likelihood of spontaneous resolution of symptoms—patients with more severe symptoms are less likely to resolve their disease spontaneously. The primary goal of antibiotic therapy is to eradicate bacteria from the site of infection, which, in turn, helps (1) return the sinuses back to health; (2) decrease the duration of symptoms to allow patients to resume daily activities more quickly; (3) prevent severe complications such as meningitis and brain abscess; and (4) decrease the development of chronic disease. Severe or life-threatening infections with or without complications are rare, and are not addressed in these guidelines. Prior antibiotic use is a major risk factor associated with the development of infection with antimicrobial-resistant strains. Because recent antimicrobial exposure increases the risk of carriage of and infection due to resistant organisms, antimicrobial therapy should be based upon the patient’s history of recent antibiotic use. The panel’s guidelines, therefore, stratify patients according to antibiotic exposure in the previous 4 to 6 weeks. Lack of response to therapy at ≥72 hours is an arbitrary time established to define treatment failures. Clinicians should monitor the response to antibiotic therapy, which may include instructing the patient to call the office or clinic if symptoms persist or worsen over the next few days. The predicted bacteriologic and clinical efficacy of antibiotics in adults and children has been determined according to mathematical modeling of ABRS developed by Michael Poole, MD, PhD, based on pathogen distribution, resolution rates without treatment, and in vitro microbiologic activity. Antibiotics can be placed into the following relative rank order of predicted clinical efficacy for adults: 90% to 92% = respiratory fluoroquinolones (gatifloxacin, levofloxacin, moxifloxacin), ceftriaxone, high-dose amoxicillin/clavulanate (4 g/250 mg/day), and amoxicillin/clavulanate (1.75 g/250 mg/day); 83% to 88% = high-dose amoxicillin (4 g/day), amoxicillin (1.5 g/day), cefpodoxime proxetil, cefixime (based on and coverage), cefuroxime axetil, cefdinir, and TMP/SMX; 77% to 81% = doxycycline, clindamycin (based on gram-positive coverage only), azithromycin, clarithromycin and erythromycin, and telithromycin; 65% to 66% = cefaclor and loracarbef. The predicted spontaneous resolution rate in patients with a clinical diagnosis of ABRS is 62%. Antibiotics can be placed into the following relative rank order of predicted clinical efficacy in children with ABRS: 91% to 92% = ceftriaxone, high-dose amoxicillin/clavulanate (90 mg/6.4 mg per kg per day) and amoxicillin/clavulanate (45 mg/6.4 mg per kg per day); 82% to 87% = high-dose amoxicillin (90 mg/kg per day), amoxicillin (45 mg/kg per day), cefpodoxime proxetil, cefixime (based on and coverage only), cefuroxime axetil, cefdinir, and TMP/SMX; and 78% to 80% = clindamycin (based on gram-positive coverage only), cefprozil, azithromycin, clarithromycin, and erythromycin; 67% to 68% = cefaclor and loracarbef. The predicted spontaneous resolution rate in untreated children with a presumed diagnosis of ABRS is 63%. Recommendations for initial therapy for adult patients with mild disease (who have not received antibiotics in the previous 4 to 6 weeks) include the following choices: amoxicillin/clavulanate (1.75 to 4 g/250 mg per day), amoxicillin (1.5 to 4 g/day), cefpodoxime proxetil, cefuroxime axetil, or cefdinir. While TMP/SMX, doxycycline, azithromycin, clarithromycin, erythromycin, or telithromycin may be considered for patients with β-lactam allergies, bacteriologic failure rates of 20% to 25% are possible. Failure to respond to antimicrobial therapy after 72 hours should prompt either a switch to alternate antimicrobial therapy or reevaluation of the patient (see Table 4).When a change in antibiotic therapy is made, the clinician should consider the limitations in coverage of the initial agent. Recommendations for initial therapy for adults with mild disease who have received antibiotics in the previous 4 to 6 weeks adults with moderate disease include the following choices: respiratory fluoroquinolone (eg, gatifloxacin, levofloxacin, moxifloxacin) or high-dose amoxicillin/clavulanate (4 g/250 mg per day). The widespread use of respiratory fluoroquinolones for patients with milder disease may promote resistance of a wide spectrum of organisms to this class of agents. Ceftriaxone (parenteral, 1 to 2 g/day for 5 days) or combination therapy with adequate gram-positive and negative coverage may also be considered. Examples of appropriate regimens of combination therapy include high-dose amoxicillin or clindamycin plus cefixime, or high-dose amoxicillin or clindamycin plus rifampin. While the clinical effectiveness of ceftriaxone and these combinations for ABRS is unproven; the panel considers these reasonable therapeutic options based on the spectrum of activity of these agents and on data extrapolated from acute otitis media studies. Rifampin should not be used as monotherapy, casually, or for longer than 10 to 14 days, as resistance quickly develops to this agent. Rifampin is also a well-known inducer of several cytochrome p450 isoenzymes and therefore has a high potential for drug interactions. Failure of a patient to respond to antimicrobial therapy after 72 hours of therapy should prompt either a switch to alternate antimicrobial therapy or reevaluation of the patient (see Table 4). When a change in antibiotic therapy is made, the clinician should consider the limitations in coverage of the initial agent. Patients who have received effective antibiotic therapy and continue to be symptomatic may need further evaluation. A CT scan, fiberoptic endoscopy or sinus aspiration and culture may be necessary. Recommendations for initial therapy for children with disease and who have received antibiotics in the previous 4 to 6 weeks include the following: high-dose amoxicillin/clavulanate (90 mg/6.4 mg per kg per day), amoxicillin (90 mg/kg per day), cefpodoxime proxetil, cefuroxime axetil, or cefdinir. TMP/SMX, azithromycin, clarithromycin, or erythromycin is recommended if the patient has a history of immediate Type I hypersensitivity reaction to β-lactams. These antibiotics have limited effectiveness against the major pathogens of ABRS and bacterial failure of 20% to 25% is possible. The clinician should differentiate an immediate hypersensitivity reaction from other less dangerous side effects. Children with immediate hypersensitivity reactions to β-lactams may need: desensitization, sinus cultures, or other ancillary procedures and studies. Children with other types of reactions and side effects may tolerate one specific β-lactam, but not another. Failure to respond to antimicrobial therapy after 72 hours should prompt either a switch to alternate antimicrobial therapy or reevaluation of the patient (see Table 5).When a change in antibiotic therapy is made, the clinician should consider the limitations in coverage of the initial agent. The recommended initial therapy for children with disease who received antibiotics in the previous 4 to 6 weeks children with disease is high-dose amoxicillin/clavulanate (90 mg/6.4 mg per kg per day). Cefpodoxime proxetil, cefuroxime axetil, or cefdinir may be used if there is a penicillin allergy (eg, penicillin rash); in such instances, cefdinir is preferred because of high patient acceptance. TMP/SMX, azithromycin, clarithromycin, or erythromycin is recommended if the patient is β-lactam allergic, but these do not provide optimal coverage. Clindamycin is appropriate if is identified as a pathogen. Ceftriaxone (parenteral, 50 mg/kg per day for 5 days) or combination therapy with adequate gram-positive and -negative coverage may also be considered. Examples of appropriate regimens of combination therapy include high-dose amoxicillin or clindamycin plus cefixime, or high-dose amoxicillin or clindamycin plus rifampin. The clinical effectiveness of ceftriaxone and these combinations for ABRS is unproven; the panel considers these reasonable therapeutic options based on spectrum of activity and on data extrapolated from acute otitis media studies. Rifampin should not be used as monotherapy, casually, or for longer than 10 to 14 days as resistance quickly develops to this agent. Failure to respond to antimicrobial therapy after 72 hours of therapy should prompt either a switch to alternate antimicrobial therapy or reevaluation of the patient (see Table 5). When a change in antibiotic therapy is made, the clinician should consider the limitations in coverage of the initial agent. Patients who have received effective antibiotic therapy and continue to be symptomatic may need further evaluation. A CT scan, fiberoptic endoscopy or sinus aspiration and culture may be necessary.
鼻窦与过敏健康合作组织制定的急性细菌性鼻窦炎(ABRS)治疗指南最初于2000年发布。这些指南旨在:(1)教育临床医生和患者(或患者家属)了解病毒性和细菌性鼻窦炎的区别;(2)减少非细菌性鼻/鼻窦疾病的抗生素使用;(3)为ABRS的诊断和最佳治疗提供建议;(4)在可能发生细菌感染时促进使用适当的抗生素治疗;(5)描述目前对药代动力学和药效学的理解以及它们与抗菌治疗效果的关系。此处更新原始指南,以纳入有关管理原则、抗菌药物敏感性模式和治疗选择的最新信息。
在美国,估计每年发生2000万例ABRS。根据国家门诊医疗调查(NAMCS)数据,鼻窦炎是开具抗生素处方的第五大常见诊断疾病。2002年,鼻窦炎分别占所有儿科和成人抗生素处方的9%和21%。鼻窦炎的主要诊断每年在美国导致约35亿美元的支出。
ABRS的定义和诊断:ABRS通常先出现病毒性上呼吸道感染(URI)。过敏、外伤、牙科感染或其他导致鼻和鼻窦炎症的因素也可能使个体易患ABRS。患有“普通感冒”(病毒性URI)的患者通常会报告以下一些症状组合:打喷嚏、流鼻涕、鼻塞、嗅觉减退/嗅觉丧失、面部压迫感、鼻后滴漏、喉咙痛、咳嗽、耳部胀满感、发热和肌痛。鼻分泌物颜色或特征的改变不是细菌感染的特异性体征。在病毒性URI病程中的任何时候都可能发生细菌重叠感染。如果疾病在10天后仍存在,则发生细菌重叠感染的风险更大。由于可能存在不符合这种典型病程“规范”的情况,临床医生在使用这些指南时需要依靠他们的临床判断。然而,一般来说,对于症状持续10天未改善或在5至7天后恶化的病毒性URI症状的成人或儿童,可作出ABRS的诊断。可能会出现以下部分或全部体征和症状:鼻分泌物、鼻塞、面部压迫感/疼痛(尤其是单侧且集中在特定鼻窦区域时)、鼻后引流、嗅觉减退/嗅觉丧失、发热、咳嗽、疲劳、上颌牙痛和耳部压迫感/胀满感。体格检查在ABRS诊断中提供的信息有限。虽然有时有帮助,但对于ABRS病例,普通X线平片、计算机断层扫描(CT)和磁共振成像扫描并非必需。
ABRS的微生物学:从ABRS患者上颌窦分离出的最常见细菌种类是 、 和 ,后者在儿童中更常见。其他链球菌种类、厌氧菌和 导致一小部分病例。
ABRS中的细菌耐药性:在美国, 对青霉素不敏感和对其他药物类别耐药的患病率不断上升,最近的研究显示15%为青霉素中介型,25%为青霉素耐药型。 对大环内酯类和甲氧苄啶/磺胺甲恶唑(TMP/SMX)的耐药也很常见。产生β-内酰胺酶的 分离株患病率约为30%,而基本上所有 分离株都产生β-内酰胺酶。 对TMP/SMX的耐药也很常见。
ABRS抗菌治疗指南:这些指南适用于成人和儿童。为ABRS选择抗生素治疗时,临床医生应考虑疾病的严重程度、疾病的进展速度和近期的抗生素暴露情况。现在指南将ABRS患者分为两大类:(1)过去4至6周内未接受过抗生素治疗且症状较轻的患者;(2)过去4至6周内接受过抗生素治疗的轻症患者或无论近期抗生素暴露情况如何的中度疾病患者。疾病严重程度的差异并不意味着感染了耐药病原体。相反,这种术语表示对可能的治疗失败的接受程度和症状自发缓解的可能性的相对程度——症状较严重的患者自发缓解疾病的可能性较小。抗生素治疗的主要目标是从感染部位根除细菌,这反过来有助于:(1)使鼻窦恢复健康;(2)缩短症状持续时间,使患者能更快恢复日常活动;(3)预防严重并发症,如脑膜炎和脑脓肿;(4)减少慢性病的发生。伴有或不伴有并发症的严重或危及生命的感染很少见,本指南未涉及。先前使用抗生素是与抗菌药物耐药菌株感染发生相关的主要危险因素。由于近期的抗菌药物暴露增加了携带耐药菌和感染耐药菌的风险,抗菌治疗应基于患者近期的抗生素使用史。因此,专家组的指南根据患者在过去4至6周内的抗生素暴露情况对患者进行分层。≥72小时对治疗无反应是定义治疗失败的一个任意设定的时间。临床医生应监测抗生素治疗的反应,这可能包括指示患者如果症状在接下来几天持续或恶化就打电话到办公室或诊所。根据医学博士迈克尔·普尔基于病原体分布、未经治疗的缓解率和体外微生物学活性建立的ABRS数学模型,已确定了成人和儿童抗生素的预测细菌学和临床疗效。抗生素可按以下成人预测临床疗效的相对排序:90%至92% = 呼吸喹诺酮类(加替沙星、左氧氟沙星、莫西沙星)、头孢曲松、高剂量阿莫西林/克拉维酸(4g/250mg/天)和阿莫西林/克拉维酸(1.75g/250mg/天);83%至88% = 高剂量阿莫西林(4g/天)、阿莫西林(1.5g/天)、头孢泊肟酯、头孢克肟(基于 和 覆盖范围)、头孢呋辛酯、头孢地尼和TMP/SMX;77%至81% = 多西环素、克林霉素(仅基于革兰氏阳性菌覆盖范围)、阿奇霉素、克拉霉素、红霉素和泰利霉素;65%至66% = 头孢克洛和氯碳头孢。临床诊断为ABRS的患者预测自发缓解率为62%。ABRS儿童患者抗生素可按以下预测临床疗效的相对排序:91%至92% = 头孢曲松、高剂量阿莫西林/克拉维酸(90mg/6.4mg/每千克每天)和阿莫西林/克拉维酸(45mg/6.4mg/每千克每天);82%至87% = 高剂量阿莫西林(90mg/千克每天)、阿莫西林(45mg/千克每天)、头孢泊肟酯、头孢克肟(仅基于 和 覆盖范围)、头孢呋辛酯、头孢地尼和TMP/SMX;78%至80% = 克林霉素(仅基于革兰氏阳性菌覆盖范围)、头孢丙烯、阿奇霉素、克拉霉素和红霉素;67%至68% = 头孢克洛和氯碳头孢。未经治疗的疑似ABRS儿童患者预测自发缓解率为63%。对过去4至6周内未接受过抗生素治疗的轻症成年患者初始治疗的建议包括以下选择:阿莫西林/克拉维酸(1.75至4g/250mg/天)、阿莫西林(1.5至4g/天)、头孢泊肟酯、头孢呋辛酯或头孢地尼。虽然对于β-内酰胺类过敏的患者可考虑使用TMP/SMX、多西环素、阿奇霉素、克拉霉素、红霉素或泰利霉素,但细菌学失败率可能为20%至25%。72小时后对抗菌治疗无反应应促使更换为替代抗菌治疗或对患者进行重新评估(见表4)。当进行抗生素治疗变更时,临床医生应考虑初始药物覆盖范围的局限性。对过去4至6周内接受过抗生素治疗的轻症成年患者以及中度疾病成年患者初始治疗的建议包括以下选择:呼吸喹诺酮类(如加替沙星、左氧氟沙星、莫西沙星)或高剂量阿莫西林/克拉维酸(4g/250mg/天)。将呼吸喹诺酮类广泛用于病情较轻的患者可能会促使多种生物体对这类药物产生耐药性。也可考虑头孢曲松(胃肠外给药,1至2g/天,共5天)或具有足够革兰氏阳性菌和阴性菌覆盖范围的联合治疗。联合治疗的合适方案示例包括高剂量阿莫西林或克林霉素加头孢克肟,或高剂量阿莫西林或克林霉素加利福平。虽然头孢曲松和这些联合治疗对ABRS的临床有效性尚未得到证实;但专家组基于这些药物的活性谱和从急性中耳炎研究推断的数据认为这些是合理的治疗选择。利福平不应随意用作单一疗法,也不应使用超过10至14天,因为该药物很快会产生耐药性。利福平也是几种细胞色素p450同工酶的著名诱导剂,因此具有很高的药物相互作用潜力。患者在治疗72小时后对抗菌治疗无反应应促使更换为替代抗菌治疗或对患者进行重新评估(见表参考文档中相应表格编号)。当进行抗生素治疗变更时,临床医生应考虑初始药物覆盖范围的局限性。接受过有效抗生素治疗但仍有症状的患者可能需要进一步评估。可能需要进行CT扫描、纤维内镜检查或鼻窦穿刺和培养。对过去4至6周内未接受过抗生素治疗的轻症儿童患者初始治疗的建议包括以下内容:高剂量阿莫西林/克拉维酸(90mg/6.4mg/每千克每天)、阿莫西林(90mg/千克每天)、头孢泊肟酯、头孢呋辛酯或头孢地尼。如果患者有对β-内酰胺类立即发生I型超敏反应的病史,则推荐使用TMP/SMX、阿奇霉素、克拉霉素或红霉素。这些抗生素对ABRS的主要病原体有效性有限,细菌学失败率可能为20%至25%。临床医生应区分立即超敏反应与其他不太危险的副作用。对β-内酰胺类有立即超敏反应的儿童可能需要:脱敏、鼻窦培养或其他辅助检查和研究。有其他类型反应和副作用的儿童可能耐受一种特定的β-内酰胺类,但不耐受另一种。72小时后对抗菌治疗无反应应促使更换为替代抗菌治疗或对患者进行重新评估(见表5)。当进行抗生素治疗变更时,临床医生应考虑初始药物覆盖范围的局限性。对过去4至6周内接受过抗生素治疗的轻症儿童患者以及中度疾病儿童患者初始治疗推荐使用高剂量阿莫西林/克拉维酸(90mg/6.4mg/每千克每天)。如果有青霉素过敏(如青霉素皮疹),可使用头孢泊肟酯、头孢呋辛酯或头孢地尼;在这种情况下,由于患者接受度高,首选头孢地尼。如果患者对β-内酰胺类过敏,推荐使用TMP/SMX、阿奇霉素、克拉霉素或红霉素,但这些药物不能提供最佳覆盖范围。如果鉴定出 为病原体,则克林霉素是合适的。也可考虑头孢曲松(胃肠外给药,50mg/千克每天,共5天)或具有足够革兰氏阳性菌和阴性菌覆盖范围的联合治疗。联合治疗的合适方案示例包括高剂量阿莫西林或克林霉素加头孢克肟,或高剂量阿莫西林或克林霉素加利福平。头孢曲松和这些联合治疗对ABRS的临床有效性尚未得到证实;专家组基于活性谱和从急性中耳炎研究推断的数据认为这些是合理的治疗选择。利福平不应随意用作单一疗法,也不应使用超过10至14天,因为该药物很快会产生耐药性。治疗72小时后对抗菌治疗无反应应促使更换为替代抗菌治疗或对患者进行重新评估(见表5)。当进行抗生素治疗变更时,临床医生应考虑初始药物覆盖范围的局限性。接受过有效抗生素治疗但仍有症状的患者可能需要进一步评估。可能需要进行CT扫描、纤维内镜检查或鼻窦穿刺和培养。 (文档中部分细菌名称未给出具体中文,保留原文)