Sankaranarayanan Meena, Chua Leok Poh, Ghista Dhanjoo N, Tan Yong Seng
School of Mechanical and Production Engineering, Nanyang Technological University, 63 97 98, Singapore.
Biomed Eng Online. 2005 Mar 4;4:14. doi: 10.1186/1475-925X-4-14.
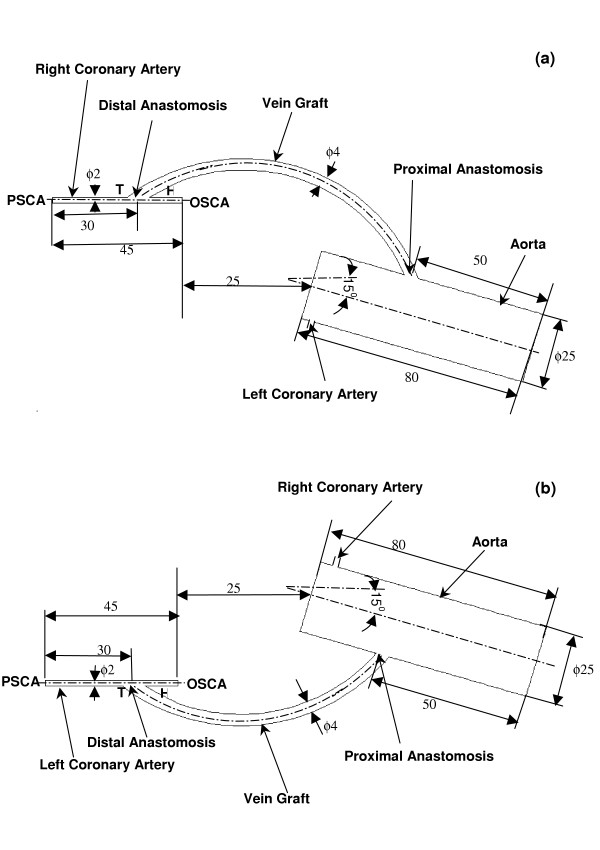
Coronary artery bypass grafting surgery is an effective treatment modality for patients with severe coronary artery disease. The conduits used during the surgery include both the arterial and venous conduits. Long- term graft patency rate for the internal mammary arterial graft is superior, but the same is not true for the saphenous vein grafts. At 10 years, more than 50% of the vein grafts would have occluded and many of them are diseased. Why do the saphenous vein grafts fail the test of time? Many causes have been proposed for saphenous graft failure. Some are non-modifiable and the rest are modifiable. Non-modifiable causes include different histological structure of the vein compared to artery, size disparity between coronary artery and saphenous vein. However, researches are more interested in the modifiable causes, such as graft flow dynamics and wall shear stress distribution at the anastomotic sites. Formation of intimal hyperplasia at the anastomotic junction has been implicated as the root cause of long- term graft failure. Many researchers have analyzed the complex flow patterns in the distal sapheno-coronary anastomotic region, using various simulated model in an attempt to explain the site of preferential intimal hyperplasia based on the flow disturbances and differential wall stress distribution. In this paper, the geometrical bypass models (aorto-left coronary bypass graft model and aorto-right coronary bypass graft model) are based on real-life situations. In our models, the dimensions of the aorta, saphenous vein and the coronary artery simulate the actual dimensions at surgery. Both the proximal and distal anastomoses are considered at the same time, and we also take into the consideration the cross-sectional shape change of the venous conduit from circular to elliptical. Contrary to previous works, we have carried out computational fluid dynamics (CFD) study in the entire aorta-graft-perfused artery domain. The results reported here focus on (i) the complex flow patterns both at the proximal and distal anastomotic sites, and (ii) the wall shear stress distribution, which is an important factor that contributes to graft patency.
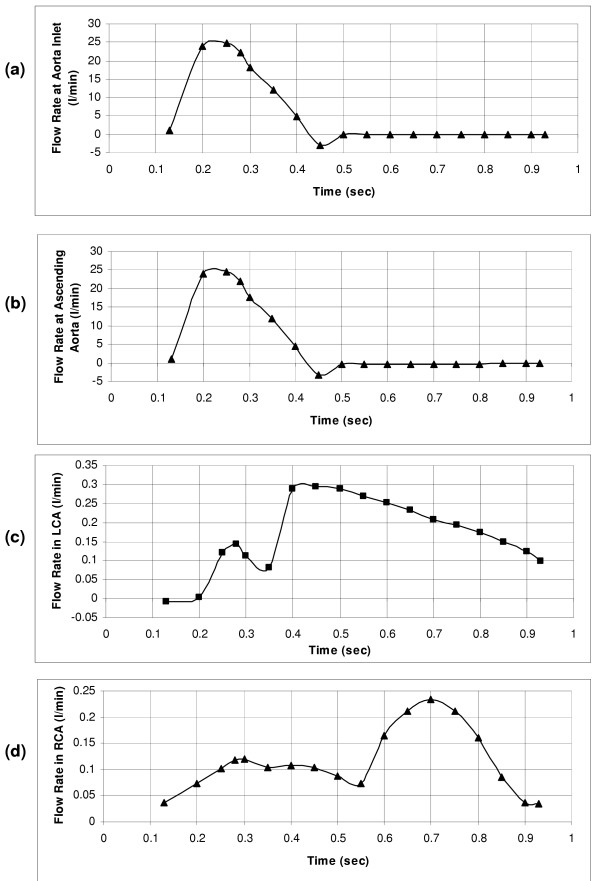
The three-dimensional coronary bypass models of the aorto-right coronary bypass and the aorto-left coronary bypass systems are constructed using computational fluid-dynamics software (Fluent 6.0.1). To have a better understanding of the flow dynamics at specific time instants of the cardiac cycle, quasi-steady flow simulations are performed, using a finite-volume approach. The data input to the models are the physiological measurements of flow-rates at (i) the aortic entrance, (ii) the ascending aorta, (iii) the left coronary artery, and (iv) the right coronary artery.
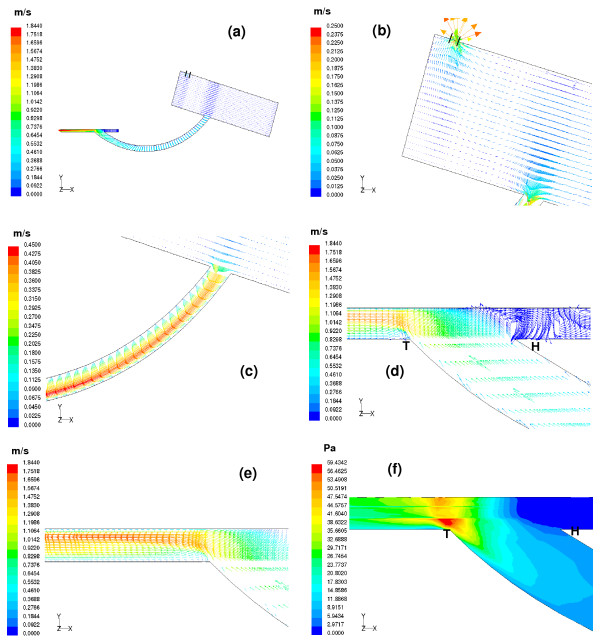
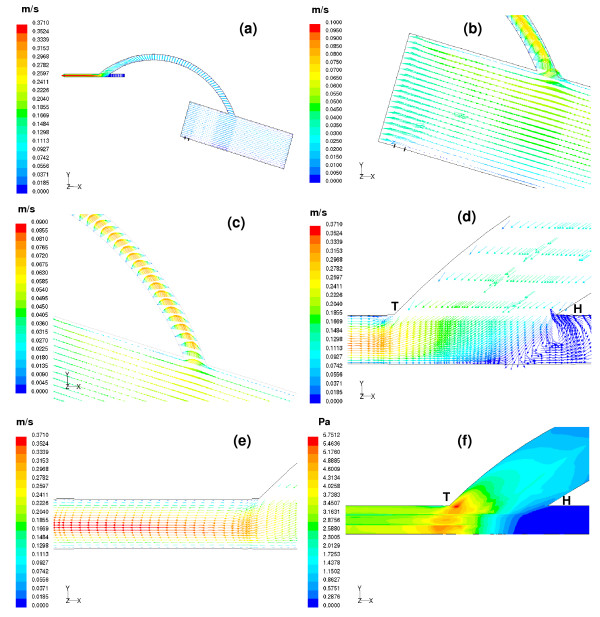
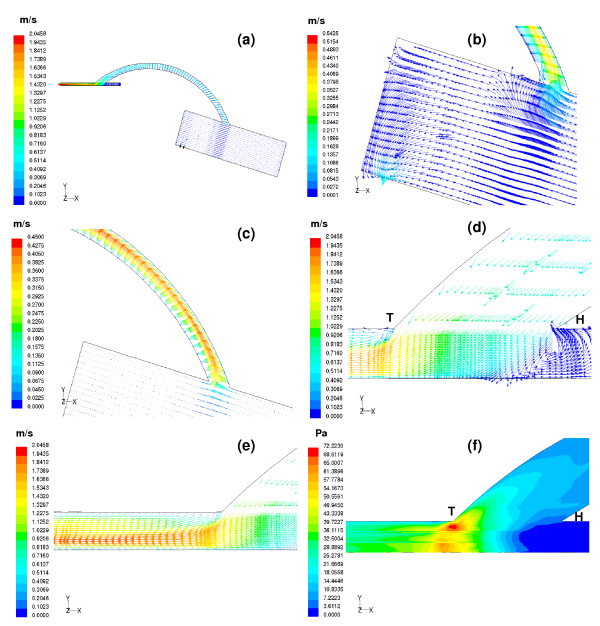
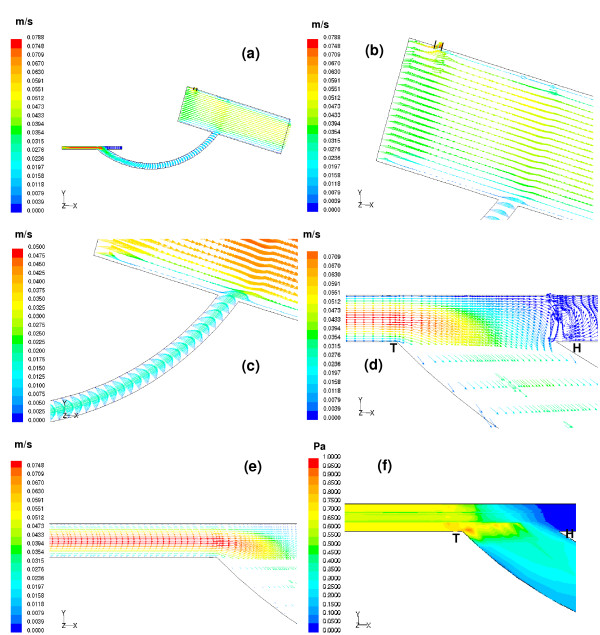
The flow field and the wall shear stress are calculated throughout the cycle, but reported in this paper at two different instants of the cardiac cycle, one at the onset of ejection and the other during mid-diastole for both the right and left aorto-coronary bypass graft models. Plots of velocity-vector and the wall shear stress distributions are displayed in the aorto-graft-coronary arterial flow-field domain. We have shown (i) how the blocked coronary artery is being perfused in systole and diastole, (ii) the flow patterns at the two anastomotic junctions, proximal and distal anastomotic sites, and (iii) the shear stress distributions and their associations with arterial disease.
The computed results have revealed that (i) maximum perfusion of the occluded artery occurs during mid-diastole, and (ii) the maximum wall shear-stress variation is observed around the distal anastomotic region. These results can enable the clinicians to have a better understanding of vein graft disease, and hopefully we can offer a solution to alleviate or delay the occurrence of vein graft disease.
冠状动脉搭桥手术是治疗严重冠状动脉疾病患者的一种有效治疗方式。手术中使用的血管桥包括动脉桥和静脉桥。乳内动脉桥的长期通畅率较高,但隐静脉桥的情况并非如此。10年后,超过50%的静脉桥会发生闭塞,其中许多还会发生病变。为什么隐静脉桥经不起时间的考验?对于隐静脉桥失败的原因,人们提出了多种。有些是不可改变的,其余的是可改变的。不可改变的原因包括静脉与动脉不同的组织结构、冠状动脉与隐静脉之间的尺寸差异。然而,研究人员对可改变的原因更感兴趣,如移植血管的血流动力学和吻合部位的壁面剪应力分布。吻合口处内膜增生的形成被认为是移植血管长期失败的根本原因。许多研究人员使用各种模拟模型分析了远端隐静脉 - 冠状动脉吻合区域的复杂血流模式,试图根据血流紊乱和不同的壁面应力分布来解释内膜增生的优先发生部位。在本文中,几何搭桥模型(主动脉 - 左冠状动脉搭桥模型和主动脉 - 右冠状动脉搭桥模型)基于实际情况构建。在我们的模型中,主动脉、隐静脉和冠状动脉的尺寸模拟了手术时的实际尺寸。同时考虑近端和远端吻合口,并且我们还考虑了静脉管道从圆形到椭圆形的横截面形状变化。与以往的研究不同,我们在整个主动脉 - 移植血管 - 灌注动脉区域进行了计算流体动力学(CFD)研究。这里报告的结果重点关注(i)近端和远端吻合口处的复杂血流模式,以及(ii)壁面剪应力分布,这是影响移植血管通畅的一个重要因素。
使用计算流体动力学软件(Fluent 6.0.1)构建主动脉 - 右冠状动脉搭桥和主动脉 - 左冠状动脉搭桥系统的三维冠状动脉搭桥模型。为了更好地理解心动周期特定时刻的血流动力学,采用有限体积法进行准稳态血流模拟。输入模型的数据是(i)主动脉入口、(ii)升主动脉、(iii)左冠状动脉和(iv)右冠状动脉处的血流速率的生理测量值。
在整个心动周期中计算了流场和壁面剪应力,但本文报告了右和左主动脉 - 冠状动脉搭桥模型在心动周期的两个不同时刻的结果,一个在射血开始时,另一个在舒张中期。在主动脉 - 移植血管 - 冠状动脉流场区域显示了速度矢量图和壁面剪应力分布图。我们展示了(i)阻塞的冠状动脉在收缩期和舒张期是如何被灌注的,(ii)两个吻合口处的血流模式,近端和远端吻合口部位,以及(iii)剪应力分布及其与动脉疾病的关联。
计算结果表明(i)闭塞动脉的最大灌注发生在舒张中期,并且(ii)在远端吻合区域周围观察到最大壁面剪应力变化。这些结果可以使临床医生更好地理解静脉桥疾病,并且希望我们能够提供一种解决方案来减轻或延迟静脉桥疾病的发生。