Curley Martha A Q, Harris Sion Kim, Fraser Karen A, Johnson Rita A, Arnold John H
Critical Care and Cardiovascular Program, Children's Hospital Boston, Boston, MA, USA.
Pediatr Crit Care Med. 2006 Mar;7(2):107-14. doi: 10.1097/01.PCC.0000200955.40962.38.
To develop and test the reliability and validity of the State Behavioral Scale for use in describing sedation/agitation levels in young intubated patients supported on mechanical ventilation.
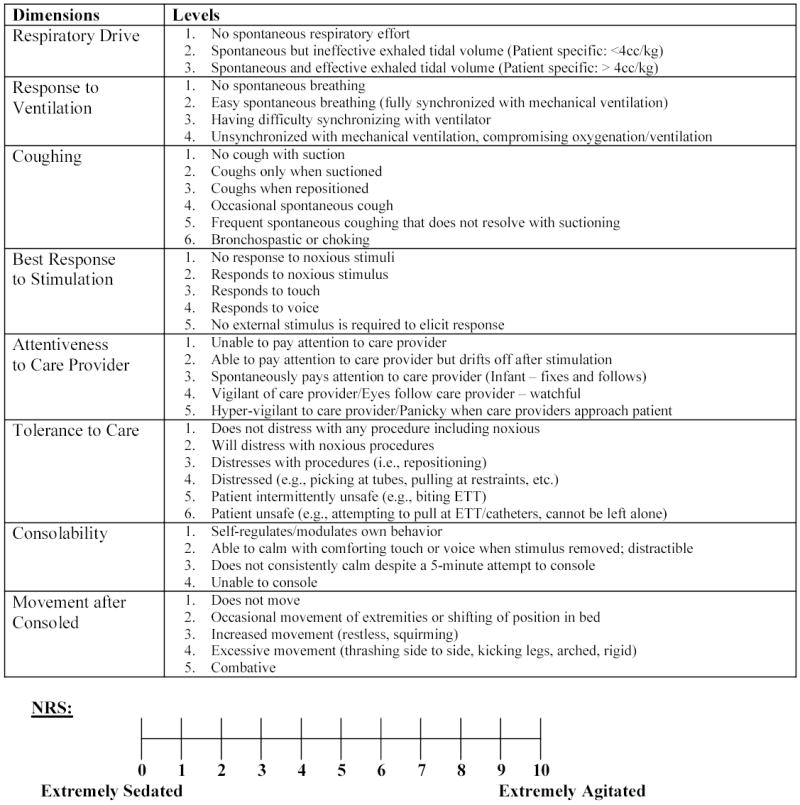
: In this prospective, psychometric evaluation, pairs of trained pediatric critical care nurse evaluators simultaneously and independently assessed a convenience sample of pediatric intensive care unit patients along eight state/behavioral dimensions and a numeric rating scale (NRS) of 0 (extremely sedated) to 10 (extremely agitated). The eight dimensions were derived from the sedation/agitation literature and expert opinion and included respiratory drive, response to ventilation, coughing, best response to stimulation, attentiveness to careprovider, tolerance to care, consolability, and movement after consoled, each with 3-5 levels.
An 18-bed pediatric medical-surgical intensive care unit and 26-bed pediatric cardiovascular intensive care unit in a university-affiliated academic children's hospital.
A total of 91 intubated mechanically ventilated patients 6 wks to 6 yrs of age provided a median of two observations (interquartile range, 1-3) for a total of 198 sets of observations. Excluded were postoperative patients or those receiving neuromuscular blockade.
Patients were observed for 1 min, and then incremental levels of stimulation were applied until patient response. After 2 mins of consoling, the state behavioral assessment and NRS were completed.
Weighted kappa and intraclass coefficients were generated to assess interrater reliability of the eight dimension and NRS ratings. Distinct state behavior profiles were empirically identified from the dimension ratings using hierarchical cluster analysis using a squared Euclidean distance measure and between-groups linkage. Construct validity of these profiles was assessed by comparing group mean NRS scores using one-way analysis of variance.
Weighted kappa scores for all 198 dimension ratings ranged from .44 to .76, indicating moderate to good interrater reliability. The intraclass coefficient of .79 was high for NRS ratings. Cluster analysis revealed five distinct state profiles, with mean NRS ratings of 1.1, 2.5, 4.0, 5.3, and 7.6, all of which differed significantly from each other (F = 75.8, p < .001), supporting the profiles' construct validity.
Based on empirically derived state behavior profiles, we have constructed the State Behavioral Scale to allow systematic description of the sedation-agitation continuum in young pediatric patients supported on mechanical ventilation. Further studies including prospective validation and describing the effect of State Behavioral Scale implementation on clinical outcomes, including the quality of sedation and length of mechanical ventilation, are warranted.
开发并测试用于描述接受机械通气的年轻插管患者镇静/躁动水平的状态行为量表的信度和效度。
在这项前瞻性心理测量评估中,经过培训的儿科重症监护护士评估人员成对地同时且独立地沿着八个状态/行为维度以及从0(深度镇静)至10(极度躁动)的数字评定量表(NRS)对儿科重症监护病房患者的便利样本进行评估。这八个维度源自镇静/躁动文献及专家意见,包括呼吸驱动、对通气的反应、咳嗽、对刺激的最佳反应、对医护人员的关注度、对护理的耐受性、安抚性以及安抚后的活动,每个维度有3至5个级别。
一所大学附属医院的一个拥有18张床位的儿科内科-外科重症监护病房以及一个拥有26张床位的儿科心血管重症监护病房。
总共91名年龄在6周龄至6岁的接受机械通气的插管患者提供了中位数为两次的观察结果(四分位间距为1至3),共计198组观察结果。排除术后患者或接受神经肌肉阻滞剂治疗的患者。
对患者观察1分钟,然后施加逐渐增加的刺激直至患者做出反应。在进行2分钟的安抚后,完成状态行为评估和NRS评定。
生成加权kappa系数和组内相关系数以评估八个维度和NRS评定的评定者间信度。使用平方欧几里得距离测度和组间连锁的层次聚类分析从维度评定中凭经验确定不同的状态行为概况。通过使用单因素方差分析比较组均值NRS分数来评估这些概况的结构效度。
所有198个维度评定的加权kappa分数范围为0.44至0.76,表明评定者间信度为中等至良好。NRS评定的组内相关系数为0.79,较高。聚类分析揭示了五种不同的状态概况,其平均NRS分数分别为1.1、2.5、4.0、5.3和7.6,所有这些概况彼此间均有显著差异(F = 75.8,p < 0.001),支持了这些概况的结构效度。
基于凭经验得出的状态行为概况,我们构建了状态行为量表,以系统描述接受机械通气的年幼儿科患者的镇静-躁动连续体。有必要开展进一步研究,包括前瞻性验证以及描述状态行为量表的实施对临床结局(包括镇静质量和机械通气时长)的影响。