Jerene Degu, Naess Are, Lindtjørn Bernt
Arba Minch Hospital, Ethiopia.
AIDS Res Ther. 2006 Apr 7;3:10. doi: 10.1186/1742-6405-3-10.
Although highly active antiretroviral therapy (HAART) reduces mortality in the developed world, it remains undocumented in resource-poor settings. We assessed the effect of HAART on patient mortality and tuberculosis incidence rate under routine clinical care conditions in Ethiopia. The objective of this study was to assess the effect of HAART on patient mortality and tuberculosis incidence rate under routine clinical care conditions in a resource-limited setting in south Ethiopia. Starting in January 2003, we followed all consecutive adult HIV infected patients who visited the HIV clinic. Since August 2003, we treated patients with HAART. Only basic laboratory services were available.
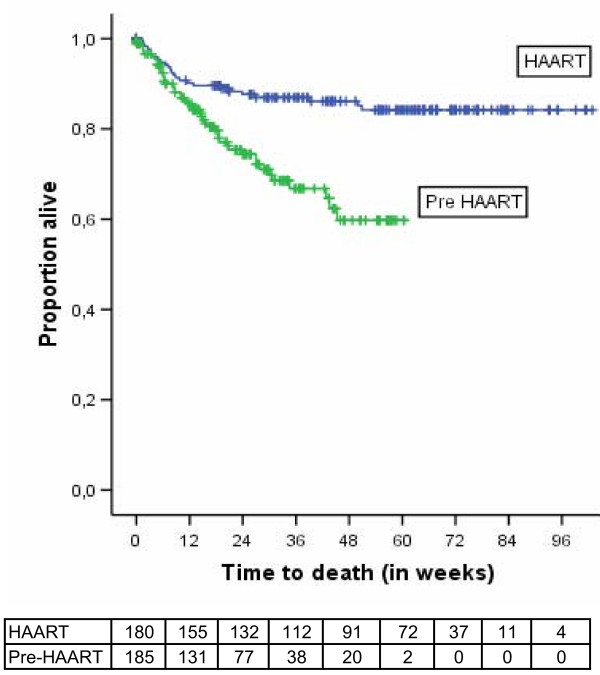
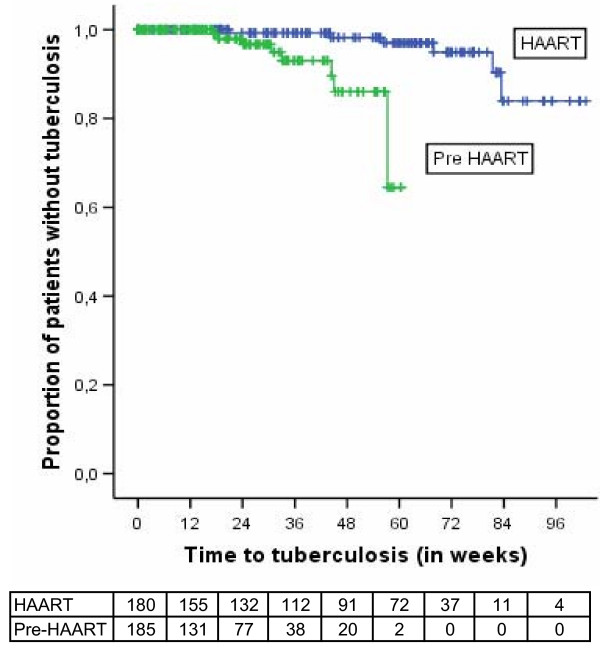
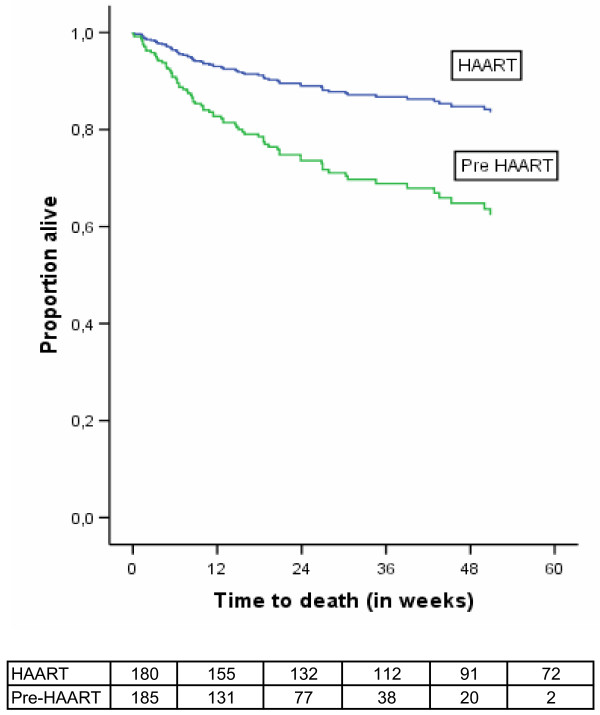
We followed 185 patients in the pre-HAART cohort and 180 patients in the HAART cohort. The mortality rate was 15.4 per 100 person-years of observation (PYO) in the HAART group and tuberculosis incidence rate was 3.7 per 100 PYO. In the pre-HAART group, the mortality rate was 58.1 per 100 PYO and the tuberculosis incidence rate was 11.1 per 100 PYO. HAART resulted in a 65% decline in mortality (adjusted hazard ratio [95%CI] = 0.35 [0.19-0.63]; P < 0.001). Tuberculosis incidence rate was lower in the HAART group (adjusted hazard ratio [95%CI] = 0.11 [0.03-0.48]; P < 0.01). Most of the deaths occurred during the first three months of treatment.
HAART improved survival and decreased tuberculosis incidence to a level similar to that achieved in the developed countries during the early years of HAART. However, both the mortality and the tuberculosis incidence rate were much higher in terms of absolute figures in this resource-limited setting. Attention should be paid to the early weeks of treatment when mortality is high. The high tuberculosis incidence rate, when coupled with the improved survival, may lead to increased tuberculosis transmission. This highlights the need for strengthening tuberculosis prevention efforts with the scale-up of treatment programmes.
尽管高效抗逆转录病毒疗法(HAART)在发达国家降低了死亡率,但在资源匮乏地区仍未得到证实。我们评估了HAART在埃塞俄比亚常规临床护理条件下对患者死亡率和结核病发病率的影响。本研究的目的是评估HAART在埃塞俄比亚南部资源有限环境下的常规临床护理条件下对患者死亡率和结核病发病率的影响。从2003年1月开始,我们对所有连续就诊于艾滋病诊所的成年HIV感染患者进行随访。自2003年8月起,我们对患者采用HAART进行治疗。当时仅有基本的实验室服务。
我们对HAART治疗前队列中的185例患者和HAART队列中的180例患者进行了随访。HAART组的死亡率为每100人年观察期(PYO)15.4例,结核病发病率为每100 PYO 3.7例。在HAART治疗前组,死亡率为每100 PYO 58.1例,结核病发病率为每100 PYO 11.1例。HAART使死亡率下降了65%(调整后风险比[95%CI]=0.35[0.19 - 0.63];P<0.001)。HAART组的结核病发病率较低(调整后风险比[95%CI]=0.11[0.03 - 0.48];P<0.01)。大多数死亡发生在治疗的前三个月。
HAART提高了生存率,并将结核病发病率降低到与HAART早期发达国家所达到的水平相似。然而,在这个资源有限地区,从绝对数字来看,死亡率和结核病发病率都要高得多。在死亡率较高的治疗早期几周应予以关注。高结核病发病率,再加上生存率的提高,可能导致结核病传播增加。这凸显了在扩大治疗方案规模的同时加强结核病预防工作的必要性。