Michiels Barbara, Philips Hilde, Coenen Samuel, Yane Fernande, Steinhauser Toon, Stuyck Sofie, Denekens Joke, Van Royen Paul
Department of Family Medicine, Centre for General Practice, University of Antwerp, University of Antwerp - Campus Drie Eiken, Universiteitsplein 1, 2610 Antwerp, Belgium.
BMC Med. 2006 Jul 10;4:17. doi: 10.1186/1741-7015-4-17.
No efficacy studies of influenza vaccination given to GPs have yet been published. Therefore, our purpose was to assess the effect of an inactivated influenza vaccine given to GPs on the rate of clinical respiratory tract infections (RTIs) and proven influenza cases (influenza positive nose and throat swabs and a 4-fold titre rise), while adjusting for important covariates.
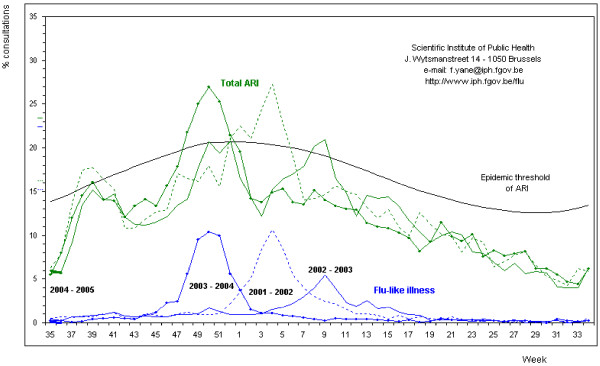
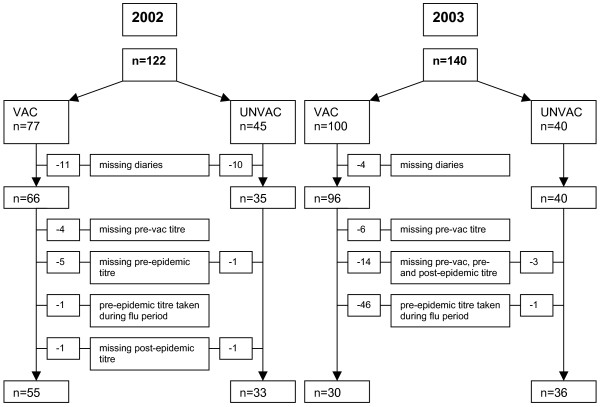
In a controlled trial during two consecutive winter periods (2002-2003 and 2003-2004) we compared (77 and 100) vaccinated with (45 and 40) unvaccinated GPs working in Flanders, Belgium. Influenza antibodies were measured immediately prior to and 3-5 weeks after vaccination, as well as after the influenza epidemic. During the influenza epidemic, GPs had to record their contact with influenza cases and their own RTI symptoms every day. If they became ill, the GPs had to take nose and throat swabs during the first 4 days. We performed a multivariate regression analysis for covariates using Generalized Estimating Equations.
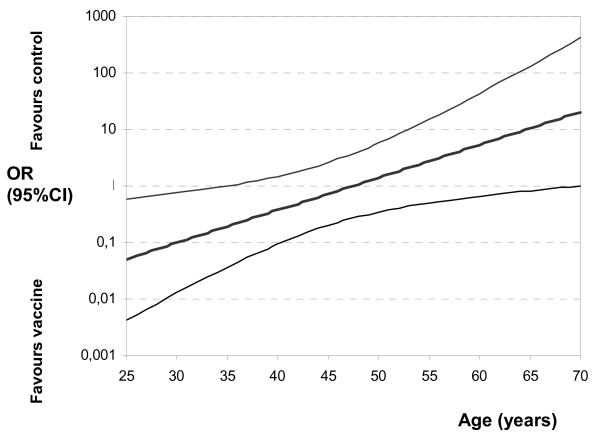
One half of the GPs (vaccinated or not) developed an RTI during the 2 influenza epidemics. During the two influenza periods, 8.6% of the vaccinated and 14.7% of the unvaccinated GPs had positive swabs for influenza (RR: 0.59; 95%CI: 0.28 - 1.24). Multivariate analysis revealed that influenza vaccination prevented RTIs and swab-positive influenza only among young GPs (ORadj: 0.35; 95%CI: 0.13 - 0.96 and 0.1; 0.01 - 0.75 respectively for 30-year-old GPs). Independent of vaccination, a low basic antibody titre against influenza (ORadj 0.57; 95%CI: 0.37 - 0.89) and the presence of influenza cases in the family (ORadj 9.24; 95%CI: 2.91 - 29) were highly predictive of an episode of swab-positive influenza.
Influenza vaccination was shown to protect against proven influenza among young GPs. GPs, vaccinated or not, who are very vulnerable to influenza are those who have a low basic immunity against influenza and, in particular, those who have family members who develop influenza.
尚无关于给全科医生接种流感疫苗的疗效研究发表。因此,我们的目的是评估给全科医生接种灭活流感疫苗对临床呼吸道感染(RTIs)发生率和确诊流感病例(流感病毒核酸检测阳性的鼻拭子和咽拭子以及四倍抗体滴度升高)的影响,同时对重要的协变量进行校正。
在连续两个冬季(2002 - 2003年和2003 - 2004年)进行的一项对照试验中,我们比较了比利时弗拉芒地区(77名和100名)接种疫苗的全科医生与(45名和40名)未接种疫苗的全科医生。在接种疫苗前、接种后3 - 5周以及流感流行后均检测流感抗体。在流感流行期间,全科医生必须每天记录他们与流感病例的接触情况以及自身的呼吸道感染症状。如果他们生病,必须在发病的前4天采集鼻拭子和咽拭子。我们使用广义估计方程对协变量进行多变量回归分析。
在两次流感流行期间,一半的全科医生(无论是否接种疫苗)发生了呼吸道感染。在两个流感流行期,接种疫苗的全科医生中有8.6%、未接种疫苗的全科医生中有14.7%的咽拭子流感病毒检测呈阳性(相对危险度:0.59;95%可信区间:0.28 - 1.24)。多变量分析显示,流感疫苗接种仅在年轻的全科医生中预防了呼吸道感染和咽拭子检测阳性的流感(对于30岁的全科医生,校正后的比值比分别为0.35;95%可信区间:0.13 - 0.96和0.1;0.01 - 0.75)。与疫苗接种无关,流感基础抗体滴度低(校正后的比值比0.57;95%可信区间:0.37 - 0.89)以及家庭中有流感病例(校正后的比值比9.24;95%可信区间:2.91 - 29)高度预测咽拭子检测阳性的流感发作。
流感疫苗接种被证明可保护年轻的全科医生预防确诊流感。无论是否接种疫苗,极易感染流感的全科医生是那些对流感基础免疫力低且特别是家庭成员感染流感的人。