Swiss Tropical Institute, Molecular Immunology, Basel, Switzerland.
PLoS Negl Trop Dis. 2007 Oct 31;1(1):e2. doi: 10.1371/journal.pntd.0000002.
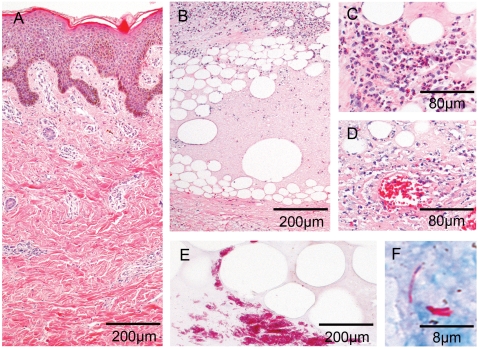
Buruli ulcer caused by Mycobacterium ulcerans is an infection of the subcutaneous tissue leading to chronic necrotising skin ulcers. The pathogenesis is associated with the cytocidal and immunosuppressive activities of a macrolide toxin. Histopathological hallmark of progressing disease is a poor inflammatory response despite of clusters of extracellular bacilli. While traditionally wide excision of the infected tissue was the standard treatment, provisional WHO guidelines now recommend an eight week pre-treatment with streptomycin and rifampicin.
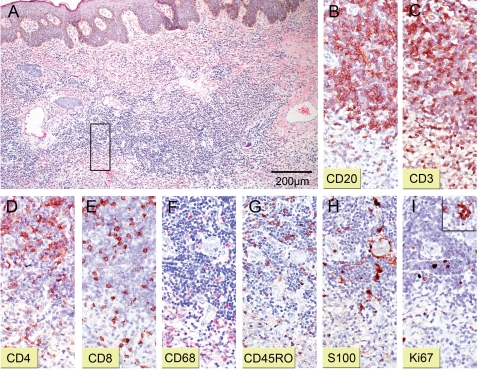
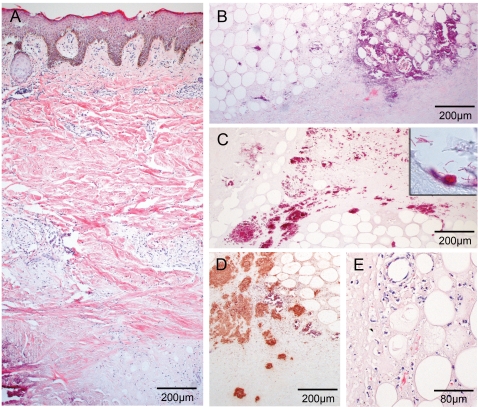
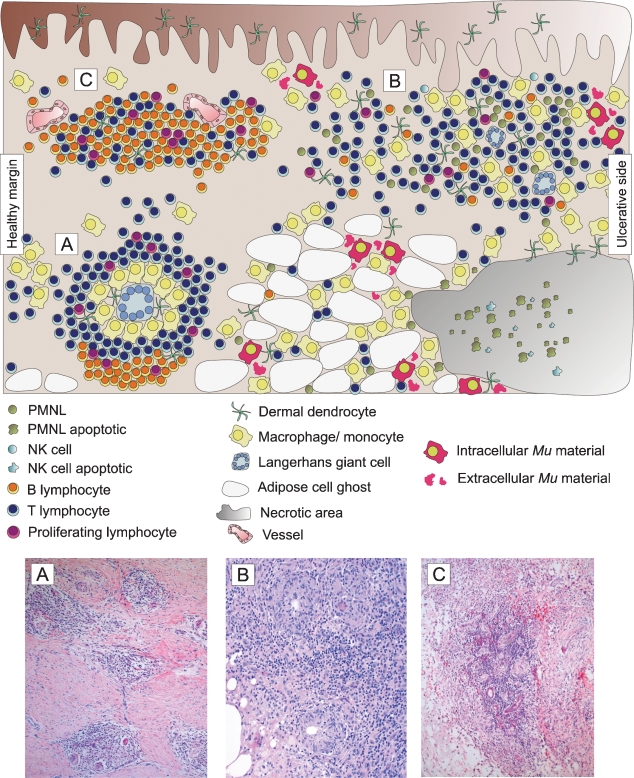
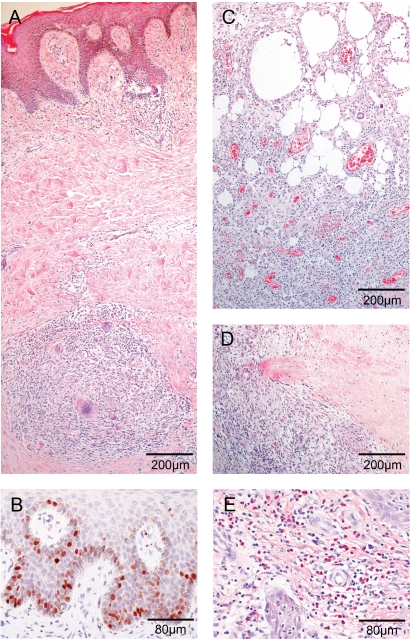
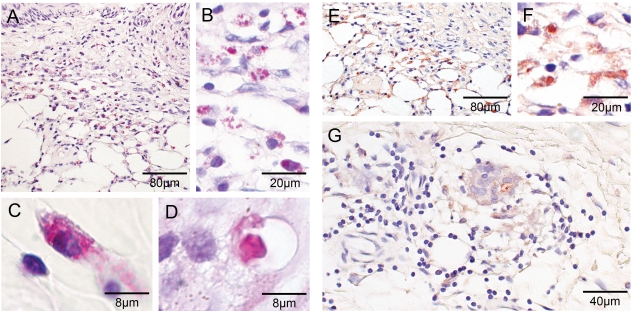
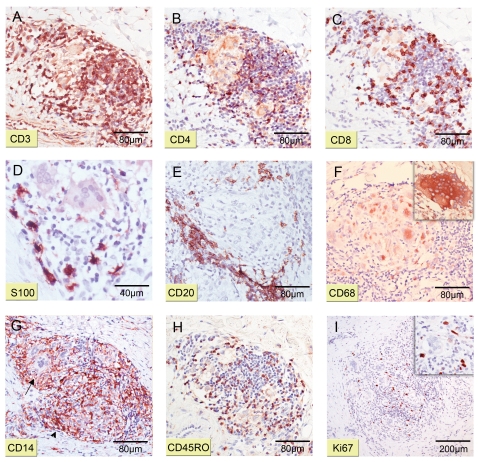
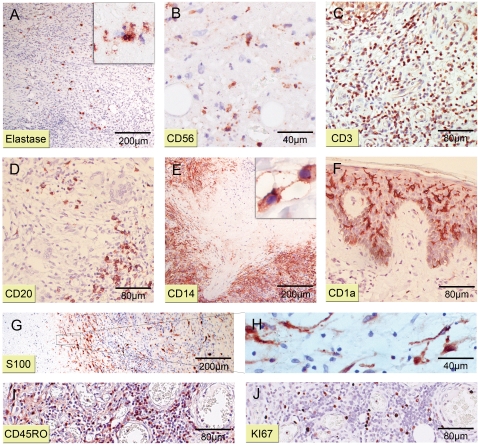
METHODOLOGY/PRINCIPAL FINDINGS: We conducted a detailed immunohistochemical analysis of tissue samples from Buruli patients who received antibiotic treatment. Cellular immune response along with bacterial load and distribution were monitored. We demonstrate that this treatment leads to the development of highly organized cellular infiltration surrounding areas of coagulative necrosis. Diffuse infiltrates, granulomas and dense lymphocyte aggregation close to vessels were observed. Mycobacterial material was primarily located inside mononuclear phagocytes and microcolonies consisting of extracellular rod-shaped mycobacteria were no longer found. In observational studies some patients showed no clinical response to antibiotic treatment. Corresponding to that, one of five lesions analysed presented with huge clusters of rod-shaped bacilli but no signs of infiltration.
CONCLUSIONS/SIGNIFICANCE: Results signify that eight weeks of antibiotic treatment reverses local immunosuppression and leads to an active inflammatory process in different compartments of the skin. Structured leukocyte infiltrates with unique signatures indicative for healing processes developed at the margins of the lesions. It remains to be analysed whether antibiotic resistance of certain strains of M. ulcerans, lacking patient compliance or poor drug quality are responsible for the absent clinical responses in some patients. In future, analysis of local immune responses could serve as a suitable surrogate marker for the efficacy of alternative treatment strategies.
由溃疡分枝杆菌引起的布鲁里溃疡是一种皮下组织感染,导致慢性坏死性皮肤溃疡。发病机制与细胞毒性和免疫抑制活性的大环内酯类毒素有关。疾病进展的组织病理学特征是尽管存在细胞外杆菌簇,但炎症反应不佳。虽然传统上广泛切除受感染的组织是标准治疗方法,但临时世界卫生组织指南现在建议在使用链霉素和利福平进行八周的预处理。
方法/主要发现:我们对接受抗生素治疗的布鲁里溃疡患者的组织样本进行了详细的免疫组织化学分析。监测细胞免疫反应、细菌负荷和分布。我们证明这种治疗会导致围绕凝固性坏死区域形成高度组织化的细胞浸润。观察到弥漫性浸润、肉芽肿和靠近血管的密集淋巴细胞聚集。分枝杆菌物质主要位于单核吞噬细胞内,不再发现由细胞外杆状分枝杆菌组成的微菌落。在观察性研究中,一些患者对抗生素治疗没有临床反应。相应地,分析的五个病变之一表现出巨大的杆状杆菌簇,但没有浸润的迹象。
结论/意义:结果表明,八周的抗生素治疗可逆转局部免疫抑制,并在皮肤的不同部位引发活跃的炎症过程。在病变边缘形成具有独特特征的结构化白细胞浸润,表明愈合过程正在进行。尚需分析某些溃疡分枝杆菌菌株的抗生素耐药性、患者顺应性差或药物质量差是否是某些患者临床反应缺失的原因。在未来,局部免疫反应分析可以作为替代治疗策略疗效的合适替代标志物。