Hui David S, Chow Benny K, Ng Susanna S, Chu Leo C Y, Hall Stephen D, Gin Tony, Sung Joseph J Y, Chan Matthew T V
Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong, People's Republic of China.
Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong, People's Republic of China; Center for Housing Innovations, The Chinese University of Hong Kong, Hong Kong, People's Republic of China.
Chest. 2009 Oct;136(4):998-1005. doi: 10.1378/chest.09-0434. Epub 2009 May 1.
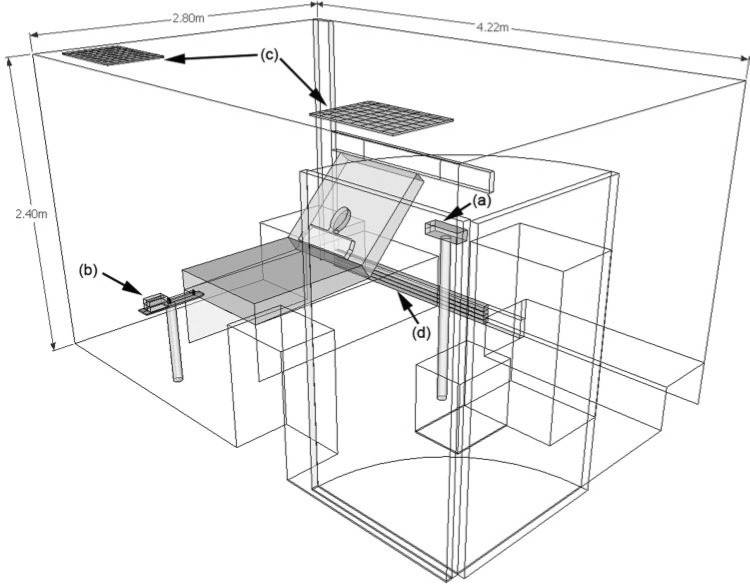
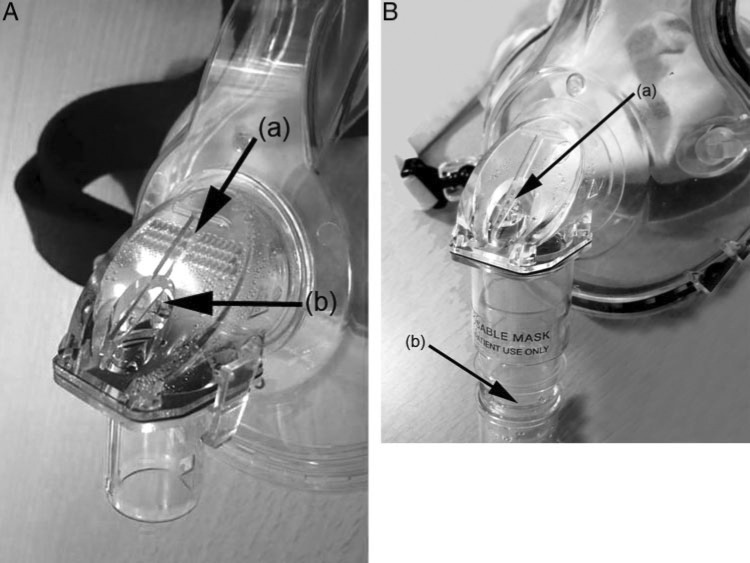
As part of our influenza pandemic preparedness, we studied the exhaled air dispersion distances and directions through two different face masks (Respironics; Murrysville, PA) attached to a human-patient simulator (HPS) during noninvasive positive-pressure ventilation (NPPV) in an isolation room with pressure of -5 Pa.
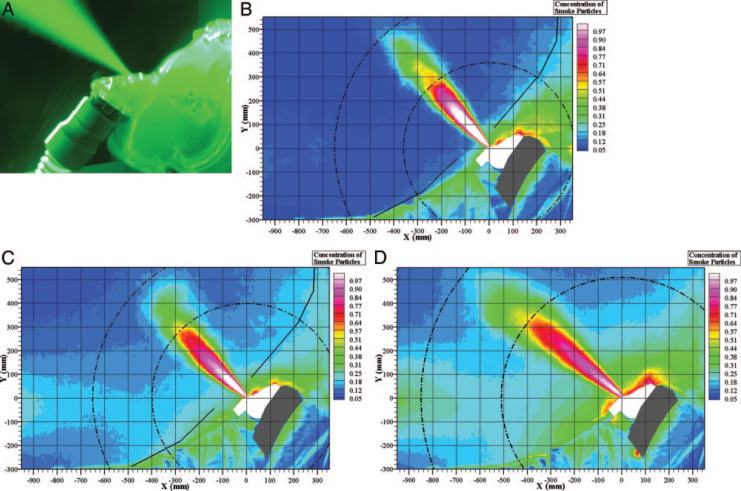
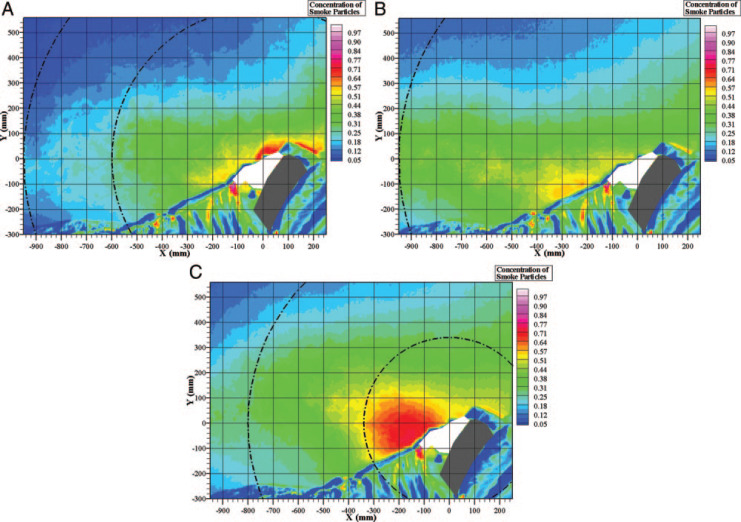
The HPS was positioned at 45 degrees on the bed and programmed to mimic mild lung injury (oxygen consumption, 300 mL/min; lung compliance, 35 mL/cm H(2)O). Airflow was marked with intrapulmonary smoke for visualization. Inspiratory positive airway pressure (IPAP) started at 10 cm H(2)O and gradually increased to 18 cm H(2)O, whereas expiratory pressure was maintained at 4 cm H(2)O. A leakage jet plume was revealed by a laser light sheet, and images were captured by high definition video. Normalized exhaled air concentration in the plume was estimated from the light scattered by the smoke particles.
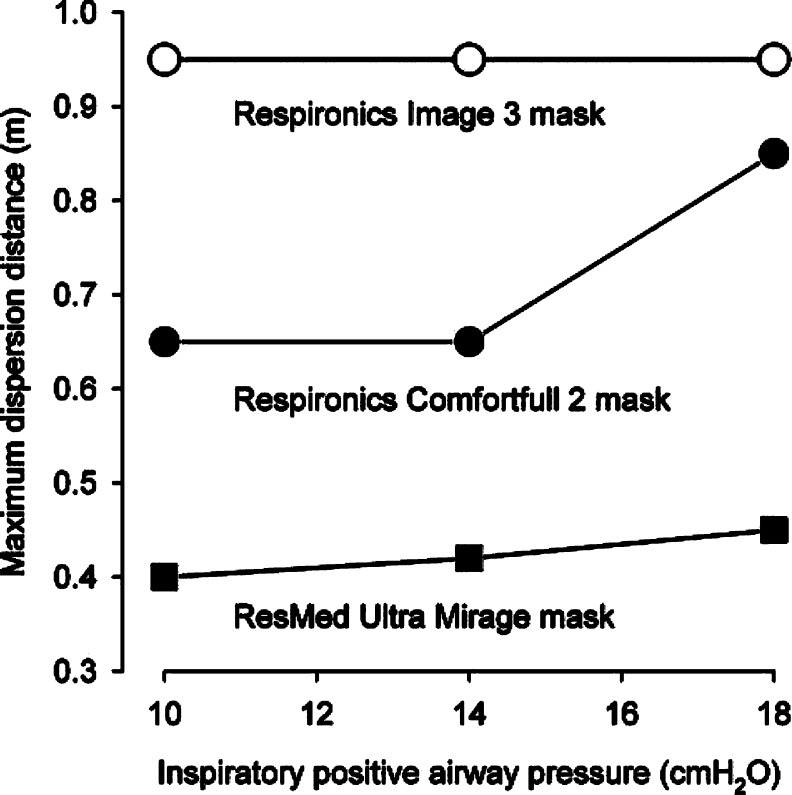
As IPAP increased from 10 to 18 cm H(2)O, the exhaled air of a low normalized concentration through the ComfortFull 2 mask (Respironics) increased from 0.65 to 0.85 m at a direction perpendicular to the head of the HPS along the median sagittal plane. When the IPAP of 10 cm H(2)O was applied via the Image 3 mask (Respironics) connected to the whisper swivel, the exhaled air dispersed to 0.95 m toward the end of the bed along the median sagittal plane, whereas higher IPAP resulted in wider spread of a higher concentration of smoke.
Substantial exposure to exhaled air occurs within a 1-m region, from patients receiving NPPV via the ComfortFull 2 mask and the Image 3 mask, with more diffuse leakage from the latter, especially at higher IPAP.
作为我们流感大流行防范工作的一部分,我们在一间压力为-5 Pa的隔离病房中,对连接到人体模拟患者(HPS)的两种不同面罩(瑞思迈公司生产,位于宾夕法尼亚州默里斯维尔)在无创正压通气(NPPV)期间呼出空气的扩散距离和方向进行了研究。
将HPS放置在床上45度角位置,并进行编程以模拟轻度肺损伤(耗氧量为300毫升/分钟;肺顺应性为35毫升/厘米水柱)。通过肺内烟雾标记气流以便可视化。吸气气道正压(IPAP)从10厘米水柱开始,逐渐增加到18厘米水柱,而呼气压力保持在4厘米水柱。用激光片光显示泄漏射流羽流,并用高清视频拍摄图像。根据烟雾颗粒散射的光估算羽流中呼出空气的归一化浓度。
随着IPAP从10厘米水柱增加到18厘米水柱,通过ComfortFull 2面罩(瑞思迈公司生产)呼出的低归一化浓度空气,在沿正中矢状面垂直于HPS头部的方向上,从0.65米增加到0.85米。当通过连接到轻声旋转接头的Image 3面罩(瑞思迈公司生产)施加10厘米水柱的IPAP时,呼出空气沿正中矢状面向床尾方向扩散到0.95米,而较高的IPAP会导致更高浓度烟雾的更广泛扩散。
使用ComfortFull 2面罩和Image 3面罩进行无创正压通气的患者,在1米范围内会有大量呼出空气暴露,后者的泄漏更分散,尤其是在较高IPAP时。