King's College London, Thames Cancer Registry, 42 Weston Street, London, SE1 3QD, UK.
BMC Public Health. 2010 Mar 25;10:157. doi: 10.1186/1471-2458-10-157.
Breast screening uptake in London is below the Government's target of 70% and we investigate whether ethnicity affects this. Information on the ethnicity for the individual women invited is unavailable, so we use an area-based method similar to that routinely used to derive a geographical measure for socioeconomic deprivation.
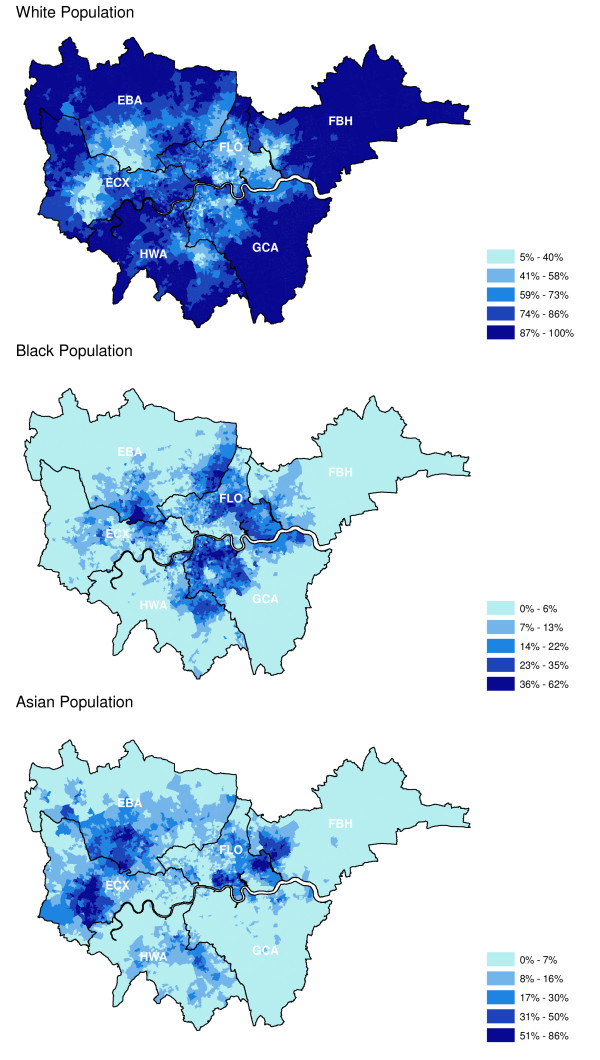
We extracted 742,786 observations on attendance for routine appointments between 2004 and 2007 collected by the London Quality Assurance Reference Centre. Each woman was assigned to a lower super output (LSOA) based on her postcode of residence. The proportions of the ethnic groups within each LSOA are known, so that the likelihood of a woman belonging to White, Black and Asian groups can be assigned. We investigated screening attendance by age group, socioeconomic deprivation using the Index of Deprivation 2004 income quintile, invitation type and breast screening service. Using logistic regression analysis we calculated odds ratios for attendance based on ethnic composition of the population, adjusting for age, socioeconomic status, the invitation type and screening service.
The unadjusted attendance odds ratios were high for the White population (OR: 3.34 95% CI [3.26-3.42]) and low for the Black population (0.13 [0.12-0.13]) and the Asian population (0.55 [0.53-0.56]). Multivariate adjustment reduced the differences, but the Black population remained below unity (0.47 [0.44-0.50]); while the White (1.30 [1.26-1.35]) and Asian populations (1.10 [1.05-1.15]) were higher. There was little difference in the attendance between age groups. Attendance was highest for the most affluent group and fell sharply with increasing deprivation. For invitation type, the routine recall was higher than the first call. There were wide variations in the attendance for different ethnic groups between the individual screening services.
Overall breast screening attendance is low in communities with large Black populations, suggesting the need to improve participation of Black women. Variations in attendance for the Asian population require further investigation at an individual screening service level.
伦敦的乳房筛查参与率低于政府设定的 70%目标,我们调查了种族是否对此有影响。由于无法获得受邀女性的种族信息,因此我们使用了一种基于区域的方法,类似于用于推导社会经济剥夺程度的地理测量方法。
我们从 2004 年至 2007 年期间由伦敦质量保证参考中心收集的常规预约中提取了 742786 条就诊记录。每位女性根据居住的邮政编码被分配到一个较低的超级输出区(LSOA)。每个 LSOA 中的种族比例是已知的,因此可以确定女性属于白种人、黑人和亚洲人群体的可能性。我们根据年龄组、2004 年收入五分位数的贫困指数、邀请类型和乳房筛查服务,调查了筛查参与率。使用逻辑回归分析,我们根据人口的种族构成计算了就诊的优势比,调整了年龄、社会经济地位、邀请类型和筛查服务的因素。
未调整的白种人就诊优势比较高(比值比:3.34,95%置信区间[3.26-3.42]),黑种人(0.13 [0.12-0.13])和亚洲人(0.55 [0.53-0.56])较低。多变量调整后,差异有所缩小,但黑人群体仍低于 1(0.47 [0.44-0.50]);而白种人(1.30 [1.26-1.35])和亚洲人(1.10 [1.05-1.15])较高。不同年龄组之间的就诊率差异不大。最富裕组的就诊率最高,随着贫困程度的增加而急剧下降。就邀请类型而言,常规召回率高于首次呼叫。不同的筛查服务之间,不同种族群体的就诊率存在很大差异。
在黑人群体较多的社区,整体乳房筛查参与率较低,表明需要提高黑人群体女性的参与度。亚洲人群体的就诊率差异需要进一步在个别筛查服务层面进行调查。