School of Computer Science and Software Engineering, University of Western Australia, Perth, Australia.
BMC Infect Dis. 2010 Jul 27;10:221. doi: 10.1186/1471-2334-10-221.
The A/H1N1 2009 influenza pandemic revealed that operational issues of school closure interventions, such as when school closure should be initiated (activation trigger), how long schools should be closed (duration) and what type of school closure should be adopted, varied greatly between and within countries. Computer simulation can be used to examine school closure intervention strategies in order to inform public health authorities as they refine school closure guidelines in light of experience with the A/H1N1 2009 pandemic.
An individual-based simulation model was used to investigate the effectiveness of school closure interventions for influenza pandemics with R0 of 1.5, 2.0 and 2.5. The effectiveness of individual school closure and simultaneous school closure were analyzed for 2, 4 and 8 weeks closure duration, with a daily diagnosed case based intervention activation trigger scheme. The effectiveness of combining antiviral drug treatment and household prophyaxis with school closure was also investigated.
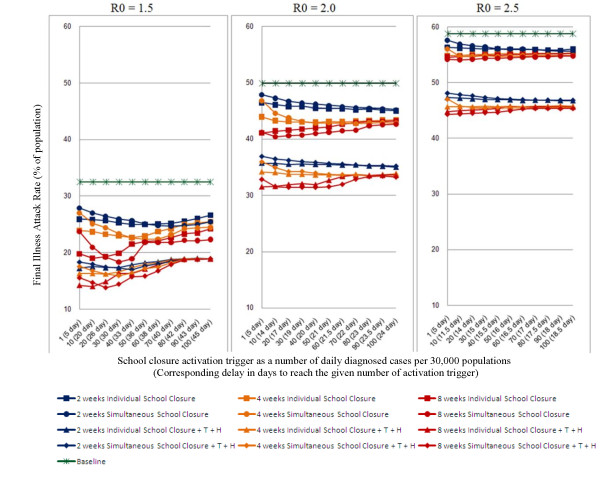
Illness attack rate was reduced from 33% to 19% (14% reduction in overall attack rate) by 8 weeks school closure activating at 30 daily diagnosed cases in the community for an influenza pandemic with R0 = 1.5; when combined with antivirals a 19% (from 33% to 14%) reduction in attack rate was obtained. For R(0) > or = 2.0, school closure would be less effective. An 8 weeks school closure strategy gives 9% (from 50% to 41%) and 4% (from 59% to 55%) reduction in attack rate for R(0) = 2.0 and 2.5 respectively; however, school closure plus antivirals would give a significant reduction (approximately 15%) in over all attack rate. The results also suggest that an individual school closure strategy would be more effective than simultaneous school closure.
Our results indicate that the particular school closure strategy to be adopted depends both on the disease severity, which will determine the duration of school closure deemed acceptable, and its transmissibility. For epidemics with a low transmissibility (R(0) < 2.0) and/or mild severity, individual school closures should begin once a daily community case count is exceeded. For a severe, highly transmissible epidemic (R(0) > or = 2.0), long duration school closure should begin as soon as possible and be combined with other interventions.
2009 年甲型 H1N1 流感大流行表明,学校关闭干预措施的实施问题,如何时启动学校关闭(激活触发)、学校应关闭多长时间(持续时间)以及应采用哪种类型的学校关闭,在国家之间和国家内部存在很大差异。计算机模拟可用于检查学校关闭干预策略,以便在根据 2009 年甲型 H1N1 大流行的经验完善学校关闭指南时为公共卫生当局提供信息。
使用基于个体的模拟模型来研究甲型 H1N1 流感大流行中学校关闭干预措施的有效性,其中基本再生数(R0)分别为 1.5、2.0 和 2.5。分析了个体学校关闭和同时关闭 2、4 和 8 周的效果,使用基于每日确诊病例的干预激活触发方案。还研究了结合抗病毒药物治疗和家庭预防措施与学校关闭的效果。
对于 R0=1.5 的流感大流行,在社区中每天确诊 30 例病例时启动 8 周的学校关闭,可以将发病率从 33%降低至 19%(总体发病率降低 14%);当与抗病毒药物联合使用时,发病率降低 19%(从 33%降至 14%)。对于 R0≥2.0,学校关闭的效果将降低。8 周的学校关闭策略可使 R0=2.0 和 2.5 的发病率分别降低 9%(从 50%降至 41%)和 4%(从 59%降至 55%);但是,学校关闭加用抗病毒药物会使总体发病率显著降低(约 15%)。结果还表明,个体学校关闭策略比同时关闭更有效。
我们的结果表明,所采用的特定学校关闭策略取决于疾病的严重程度,这将决定可接受的学校关闭持续时间;还取决于其传染性。对于传染性较低(R0<2.0)且/或严重程度较轻的流行,一旦每日社区病例数超过规定,就应开始进行个别学校关闭。对于严重且高度传染性的流行(R0≥2.0),应尽快开始长时间的学校关闭,并结合其他干预措施。