Bryce Cindy L, Chang Chung-Chou Ho, Angus Derek C, Arnold Robert M, Farrell Maxwell, Roberts Mark S
Division of General Internal Medicine, Department of Medicine, School of Medicine, University of Pittsburgh, Pittsburgh, PA 15213, USA.
J Transplant. 2010;2010:467976. doi: 10.1155/2010/467976. Epub 2010 Dec 23.
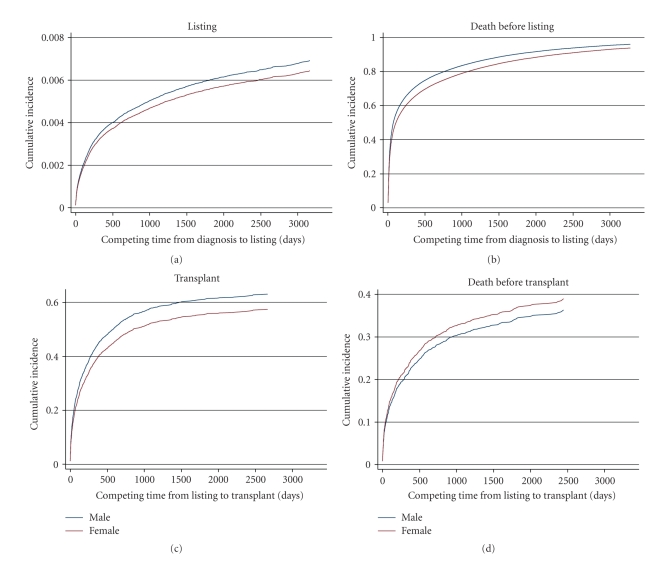
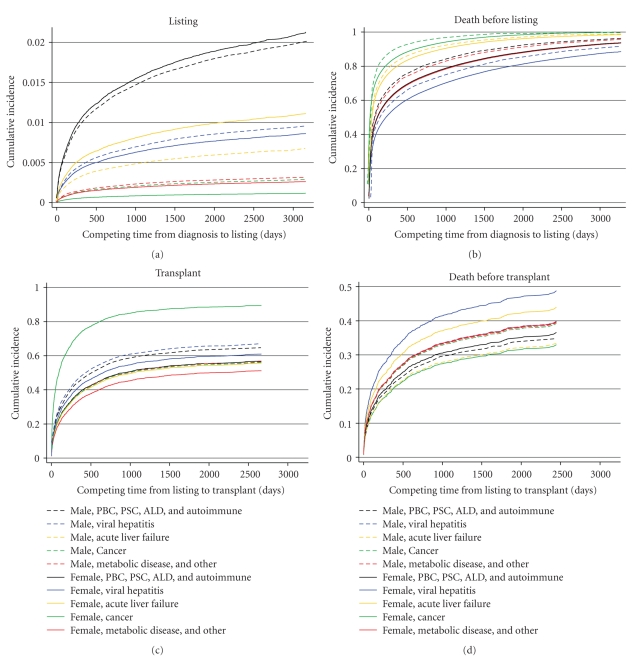
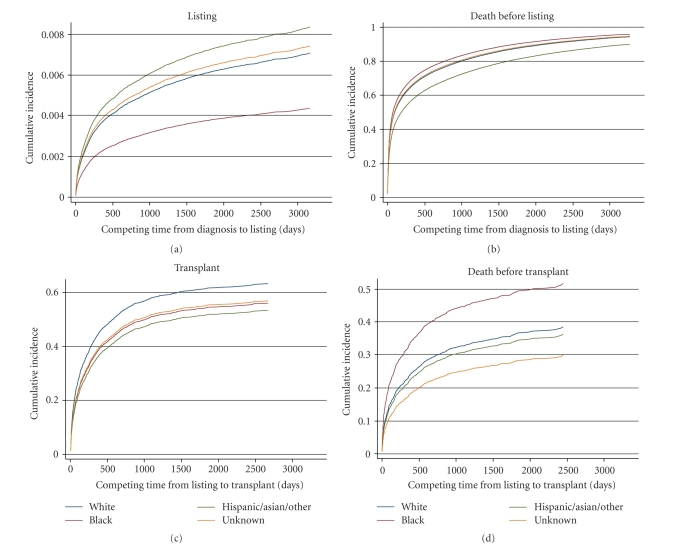
Fair allocation of organs to candidates listed for transplantation is fundamental to organ-donation policies. Processes leading to listing decisions are neither regulated nor understood. We explored whether patient characteristics affected timeliness of listing using population-based data on 144,507 adults hospitalized with liver-related disease in Pennsylvania. We linked hospitalizations to other secondary data and found 3,071 listed for transplants, 1,537 received transplants, and 57,020 died. Among candidates, 61% (n = 1,879) and 85.5% (n = 2,626) were listed within 1 and 3 years of diagnosis; 26.7% (n = 1,130) and 95% (n = 1,468) of recipients were transplanted within 1 and 3 years of listing. Using competing-risks models, we found few overall differences by sex, but both black patients and those insured by Medicare and Medicaid (combined) waited longer before being listed. Patients with combined Medicare and Medicaid insurance, as well as those with Medicaid alone, were also more likely to die without ever being listed. Once listed, the time to transplant was slightly longer for women, but it did not differ by race/ethnicity or insurance. The early time period from diagnosis to listing for liver transplantation reveals unwanted variation related to demographics that jeopardizes overall fairness of organ allocation and needs to be further explored.
向列入移植名单的候选人公平分配器官是器官捐赠政策的根本。导致列入名单决定的过程既未得到规范,也未被充分理解。我们利用宾夕法尼亚州144,507名因肝病住院的成年人的基于人群的数据,探讨了患者特征是否会影响列入名单的及时性。我们将住院数据与其他二级数据相链接,发现有3,071人被列入移植名单,1,537人接受了移植,57,020人死亡。在候选人中,61%(n = 1,879)和85.5%(n = 2,626)在诊断后的1年和3年内被列入名单;26.7%(n = 1,130)和95%(n = 1,468)的受者在列入名单后的1年和3年内接受了移植。使用竞争风险模型,我们发现总体上性别差异不大,但黑人患者以及那些由医疗保险和医疗补助(合并)承保的患者在列入名单前等待的时间更长。同时拥有医疗保险和医疗补助的患者,以及仅拥有医疗补助的患者,也更有可能在从未被列入名单的情况下死亡。一旦被列入名单,女性接受移植的时间略长,但在种族/族裔或保险方面没有差异。从诊断到列入肝移植名单的早期阶段显示出与人口统计学相关的不良差异,这危及器官分配的总体公平性,需要进一步探讨。