Division of Infectious Disease, Medical Practice Evaluation Center, Massachusetts General Hospital, Boston, Massachusetts, USA.
PLoS Med. 2012 Jan;9(1):e1001156. doi: 10.1371/journal.pmed.1001156. Epub 2012 Jan 10.
The World Health Organization (WHO) has called for the "virtual elimination" of pediatric HIV: a mother-to-child HIV transmission (MTCT) risk of less than 5%. We investigated uptake of prevention of MTCT (PMTCT) services, infant feeding recommendations, and specific drug regimens necessary to achieve this goal in Zimbabwe.
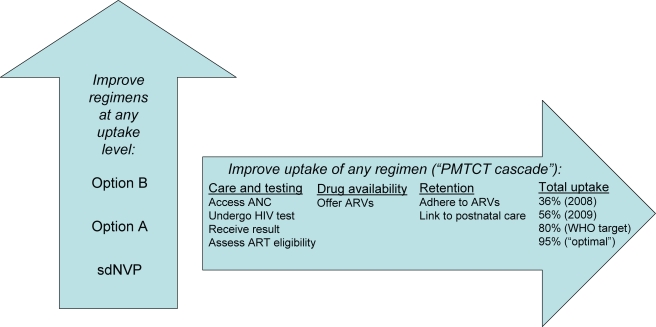
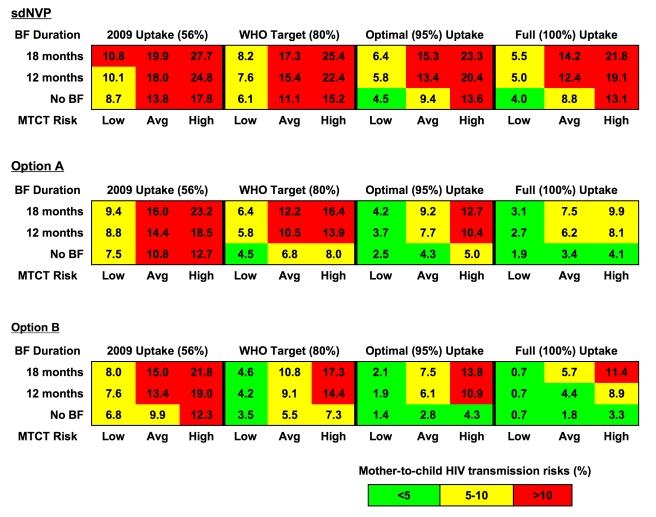
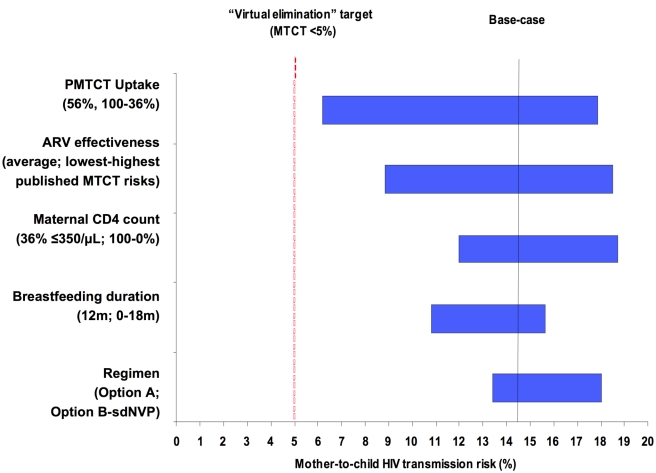
We used a computer model to simulate a cohort of HIV-infected, pregnant/breastfeeding women (mean age, 24 y; mean CD4, 451/µl; breastfeeding duration, 12 mo). Three PMTCT regimens were evaluated: (1) single-dose nevirapine (sdNVP), (2) WHO 2010 guidelines' "Option A" (zidovudine in pregnancy, infant nevirapine throughout breastfeeding for women without advanced disease, lifelong combination antiretroviral therapy for women with advanced disease), and (3) WHO "Option B" (pregnancy/breastfeeding-limited combination antiretroviral drug regimens without advanced disease; lifelong antiretroviral therapy with advanced disease). We examined four levels of PMTCT uptake (proportion of pregnant women accessing and adhering to PMTCT services): reported rates in 2008 and 2009 (36% and 56%, respectively) and target goals in 2008 and 2009 (80% and 95%, respectively). The primary model outcome was MTCT risk at weaning. The 2008 sdNVP-based National PMTCT Program led to a projected 12-mo MTCT risk of 20.3%. Improved uptake in 2009 reduced projected risk to 18.0%. If sdNVP were replaced by more effective regimens, with 2009 (56%) uptake, estimated MTCT risk would be 14.4% (Option A) or 13.4% (Option B). Even with 95% uptake of Option A or B, projected transmission risks (6.1%-7.7%) would exceed the WHO goal of less than 5%. Only if the lowest published transmission risks were used for each drug regimen, or breastfeeding duration were shortened, would MTCT risks at 95% uptake fall below 5%.
Implementation of the WHO PMTCT guidelines must be accompanied by efforts to improve access to PMTCT services, retain women in care, and support medication adherence throughout pregnancy and breastfeeding, to approach the "virtual elimination" of pediatric HIV in Zimbabwe. Please see later in the article for the Editors' Summary.
世界卫生组织(WHO)呼吁“虚拟消除”儿科艾滋病毒:母婴传播(MTCT)的风险低于 5%。我们调查了在津巴布韦实现这一目标所需的预防母婴传播(PMTCT)服务的接受程度、婴儿喂养建议以及特定药物方案。
我们使用计算机模型模拟了一组艾滋病毒感染、孕妇/哺乳期妇女(平均年龄 24 岁;平均 CD4 计数 451/µl;哺乳期 12 个月)。评估了三种 PMTCT 方案:(1)单剂量奈韦拉平(sdNVP),(2)世卫组织 2010 年指南的“方案 A”(怀孕期间使用齐多夫定,婴儿在没有晚期疾病的情况下在整个哺乳期接受奈韦拉平,晚期疾病妇女使用终身联合抗逆转录病毒疗法),以及(3)世卫组织“方案 B”(无晚期疾病的妊娠/哺乳期有限联合抗逆转录病毒药物方案;晚期疾病妇女终身抗逆转录病毒治疗)。我们检查了 PMTCT 接受程度的四个水平(接受和坚持 PMTCT 服务的孕妇比例):2008 年和 2009 年的报告率(分别为 36%和 56%)和 2008 年和 2009 年的目标(分别为 80%和 95%)。主要模型结果是断奶时的 MTCT 风险。基于 2008 年 sdNVP 的国家 PMTCT 计划导致预测的 12 个月 MTCT 风险为 20.3%。2009 年提高接受程度降低了预测风险至 18.0%。如果用更有效的方案代替 sdNVP,并且接受程度为 2009 年的 56%,则估计的 MTCT 风险将为 14.4%(方案 A)或 13.4%(方案 B)。即使接受方案 A 或 B 的比例达到 95%,预测的传播风险(6.1%-7.7%)仍将超过世卫组织的目标(小于 5%)。只有在每个药物方案中使用发表的最低传播风险,或缩短母乳喂养时间,95%接受度的 MTCT 风险才会低于 5%。
要在津巴布韦实现“虚拟消除”儿科艾滋病毒的目标,世卫组织 PMTCT 指南的实施必须伴随着努力改善 PMTCT 服务的可及性、让妇女在护理中保持地位,并在整个孕期和哺乳期支持药物依从性。请在文章稍后查看编辑摘要。