Polyvalent Intensive Care Unit, São Francisco Xavier Hospital, CHLO, Estrada do Forte do Alto do Duque, 1449-005 Lisbon, Portugal.
Crit Care. 2011 Jul 15;15(4):R169. doi: 10.1186/cc10313.
C-reactive protein (CRP) has been shown to be a valuable marker in the diagnosis of infection and in monitoring its response to antibiotics. Our objective was to evaluate serial CRP measurements after prescription of antibiotics to describe the clinical course of Community-Acquired Sepsis admitted to intensive care units (ICU).
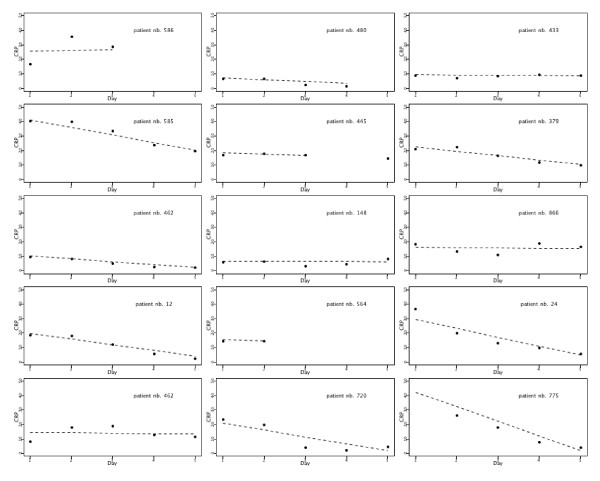
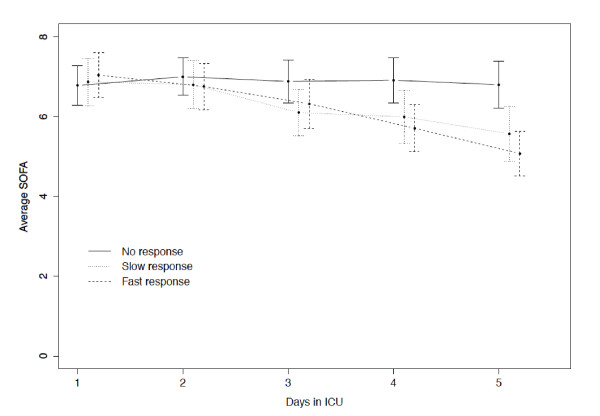
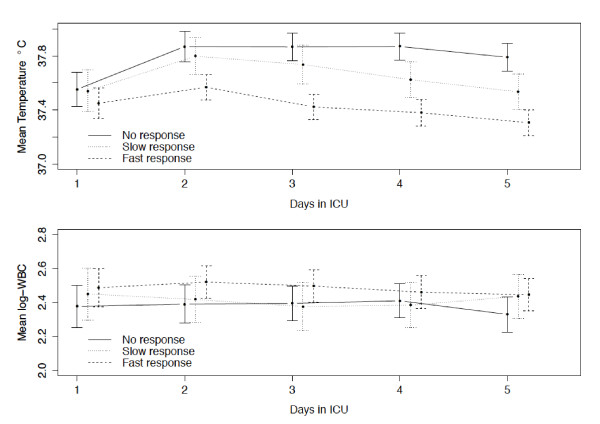
During a 12-month period a multi-center, prospective, observational study was conducted, segregating adults with Community-Acquired Sepsis. Patients were followed-up during the first five ICU days, day of ICU discharge or death and hospital outcome. CRP-ratio was calculated in relation to Day 1 CRP concentration. Patients were classified according to the pattern of CRP-ratio response to antibiotics: fast response if Day 5 CRP-ratio was < 0.4, slow response if Day 5 CRP-ratio was between 0.4 and 0.8, and no response if Day 5 CRP-ratio was > 0.8. Comparison between survivors and non-survivors was performed.
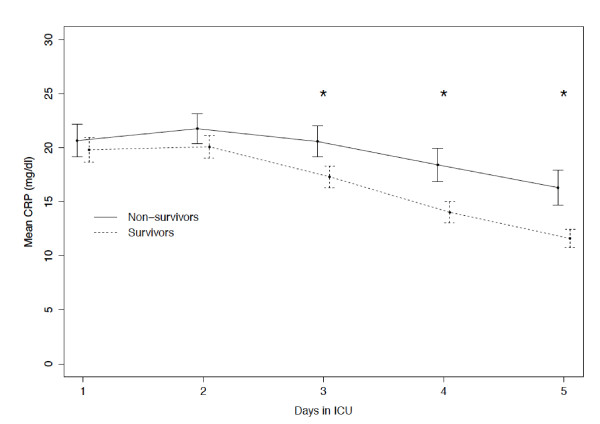
A total of 891 patients (age 60 ± 17 yrs, hospital mortality 38%) were studied. There were no significant differences between the CRP of survivors and non-survivors until Day 2 of antibiotic therapy. On the following three days, CRP of survivors was significantly lower (P < 0.001). After adjusting for the Simplified Acute Physiology Score II and severity of sepsis, the CRP course was significantly associated with mortality (ORCRP-ratio = 1.03, confidence interval 95%= (1.02, 1.04), P < 0.001). The hospital mortality of patients with fast response, slow response and no response patterns was 23%, 30% and 41%, respectively (P = 0.001). No responders had a significant increase on the odds of death (OR = 2.5, CI95% = (1.6, 4.0), P < 0.001) when compared with fast responders.
Daily CRP measurements after antibiotic prescription were useful as early as Day 3 in identification of Community-Acquired Sepsis patients with poor outcome. The rate of CRP decline during the first five ICU days was markedly associated with prognosis. The identification of the pattern of CRP-ratio response was useful in the recognition of the individual clinical course.
C 反应蛋白(CRP)已被证明是诊断感染和监测抗生素治疗反应的有价值的标志物。我们的目的是评估抗生素治疗后连续 CRP 测量值,以描述入住重症监护病房(ICU)的社区获得性败血症患者的临床病程。
在为期 12 个月的时间里,进行了一项多中心、前瞻性、观察性研究,将成人社区获得性败血症患者分开。患者在 ICU 入住的前 5 天、ICU 出院日或死亡日和住院结局进行随访。CRP 比值与第 1 天 CRP 浓度相关计算。根据 CRP-比值对抗生素反应的模式对患者进行分类:第 5 天 CRP-比值<0.4 为快速反应,第 5 天 CRP-比值在 0.4 到 0.8 之间为缓慢反应,第 5 天 CRP-比值>0.8 为无反应。对存活者和非存活者进行比较。
共纳入 891 例患者(年龄 60 ± 17 岁,住院死亡率 38%)。在抗生素治疗开始后的前 2 天,存活者和非存活者的 CRP 没有显著差异。在接下来的三天里,存活者的 CRP 明显降低(P < 0.001)。在调整简化急性生理学评分 II 和败血症严重程度后,CRP 病程与死亡率显著相关(CRP-比值=1.03,95%置信区间=(1.02,1.04),P < 0.001)。快速反应、缓慢反应和无反应模式患者的住院死亡率分别为 23%、30%和 41%(P = 0.001)。与快速反应者相比,无反应者死亡的几率显著增加(OR=2.5,95%CI=(1.6,4.0),P < 0.001)。
抗生素治疗后每日 CRP 测量值在第 3 天即可用于识别预后不良的社区获得性败血症患者。前 5 天 ICU 入住期间 CRP 下降率与预后显著相关。CRP 比值反应模式的识别有助于识别个体的临床病程。