Africa Centre for Health and Population Studies, University of KwaZulu-Natal, Somkhele, South Africa.
Popul Health Metr. 2011 Aug 5;9:47. doi: 10.1186/1478-7954-9-47.
The advent of the HIV pandemic and the more recent prevention and therapeutic interventions have resulted in extensive and rapid changes in cause-specific mortality rates in sub-Saharan Africa, and there is demand for timely and accurate cause-specific mortality data to steer public health responses and to evaluate the outcome of interventions. The objective of this study is to describe cause-specific mortality trends based on verbal autopsies conducted on all deaths in a rural population in KwaZulu-Natal, South Africa, over a 10-year period (2000-2009).
The study used population-based mortality data collected by a demographic surveillance system on all resident and nonresident members of 12,000 households. Cause of death was determined by verbal autopsy based on the standard INDEPTH/WHO verbal autopsy questionnaire. Cause of death was assigned by physician review and the Bayesian-based InterVA program.
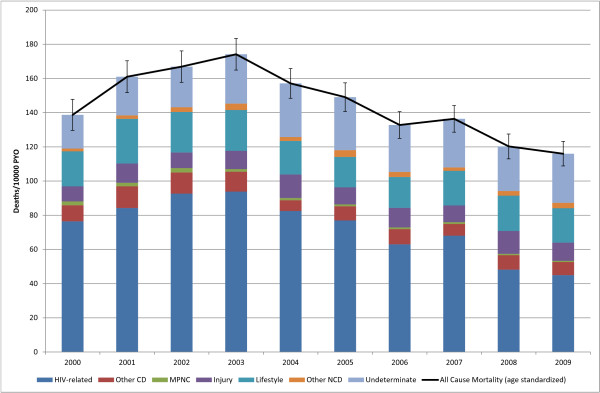
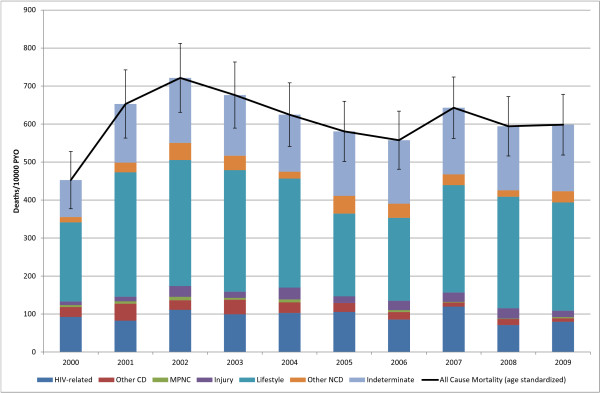
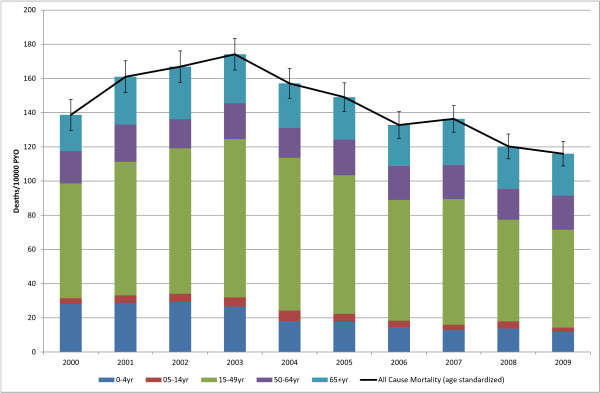
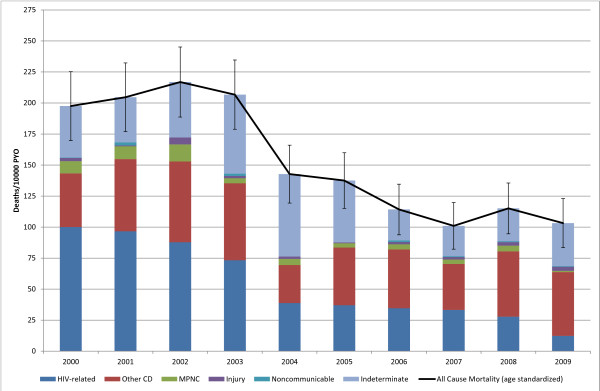
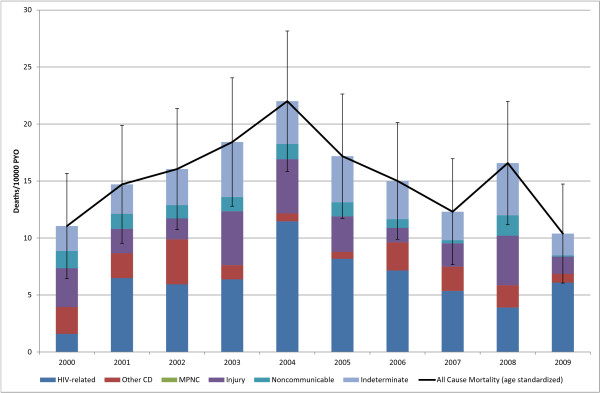
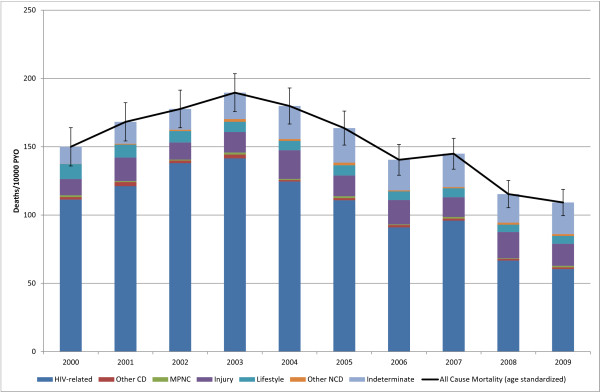
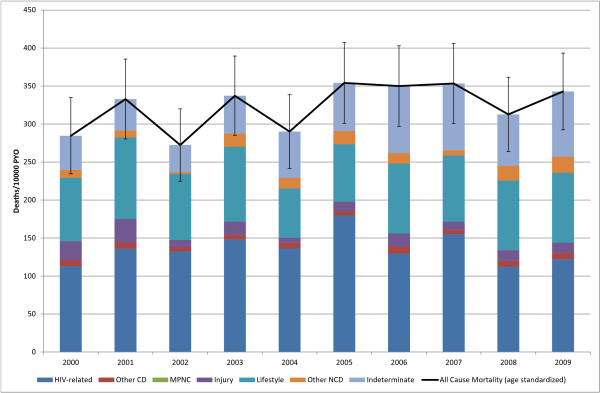
There were 11,281 deaths over 784,274 person-years of observation of 125,658 individuals between Jan. 1, 2000 and Dec. 31, 2009. The cause-specific mortality fractions (CSMF) for the population as a whole were: HIV-related (including tuberculosis), 50%; other communicable diseases, 6%; noncommunicable lifestyle-related conditions, 15%; other noncommunicable diseases, 2%; maternal, perinatal, nutritional, and congenital causes, 1%; injury, 8%; indeterminate causes, 18%. Over the course of the 10 years of observation, the CSMF of HIV-related causes declined from a high of 56% in 2002 to a low of 39% in 2009 with the largest decline starting in 2004 following the introduction of an antiretroviral treatment program into the population. The all-cause age-standardized mortality rate (SMR) declined over the same period from a high of 174 (95% confidence interval [CI]: 165, 183) deaths per 10,000 person-years observed (PYO) in 2003 to a low of 116 (95% CI: 109, 123) in 2009. The decline in the SMR is predominantly due to a decline in the HIV-related SMR, which declined in the same period from 96 (95% CI: 89, 102) to 45 (95% CI: 40, 49) deaths per 10,000 PYO.There was substantial agreement (79% kappa = 0.68 (95% CI: 0.67, 0.69)) between physician coding and InterVA coding at the burden of disease group level.
Verbal autopsy based methods enabled the timely measurement of changing trends in cause-specific mortality to provide policymakers with the much-needed information to allocate resources to appropriate health interventions.
艾滋病大流行以及最近的预防和治疗干预措施,导致撒哈拉以南非洲特定病因死亡率发生了广泛而迅速的变化,因此需要及时、准确的特定病因死亡率数据来指导公共卫生应对措施,并评估干预措施的效果。本研究的目的是描述基于南非夸祖鲁-纳塔尔省一个农村人群所有死亡的死因推断调查,在 10 年期间(2000-2009 年)特定病因死亡率趋势。
该研究使用人口监测系统收集的基于人群的死亡率数据,该系统监测了 12000 户家庭的所有居民和非居民成员。死因通过基于 INDEPTH/WHO 死因推断调查问卷的死因推断调查确定。死因由医生审查和基于贝叶斯的 InterVA 程序进行分配。
2000 年 1 月 1 日至 2009 年 12 月 31 日期间,在观察了 125658 人 784274 人年中,共有 11281 人死亡。整个人群的特定病因死亡率分数(CSMF)为:与艾滋病毒相关(包括结核病),50%;其他传染病,6%;非传染性生活方式相关疾病,15%;其他非传染性疾病,2%;孕产妇、围产期、营养和先天性疾病,1%;损伤,8%;原因不明,18%。在观察的 10 年期间,与艾滋病毒相关病因的 CSMF 从 2002 年的高峰 56%下降到 2009 年的 39%,最大降幅始于 2004 年,当时在人群中引入了抗逆转录病毒治疗方案。同期全因年龄标准化死亡率(SMR)也从 2003 年的每 10000 人年观察(PYO)174 例(95%置信区间 [CI]:165,183)的高峰下降到 2009 年的 116 例(95% CI:109,123)。SMR 的下降主要是由于与艾滋病毒相关的 SMR 下降,同期从每 10000 PYO 96 例(95% CI:89,102)下降到 45 例(95% CI:40,49)。医生编码和 InterVA 编码在疾病负担组水平上具有高度一致性(79%kappa=0.68(95% CI:0.67,0.69))。
基于死因推断调查的方法能够及时测量特定病因死亡率的变化趋势,为决策者提供急需的信息,以便将资源分配给适当的卫生干预措施。