School of Medicine, University of California San Francisco, San Francisco, California, United States of America.
PLoS One. 2011;6(11):e26983. doi: 10.1371/journal.pone.0026983. Epub 2011 Nov 9.
Short telomere length (TL) is an independent predictor of mortality in patients with coronary heart disease (CHD). However, the relationship between physical fitness and TL has not been explored in these patients.
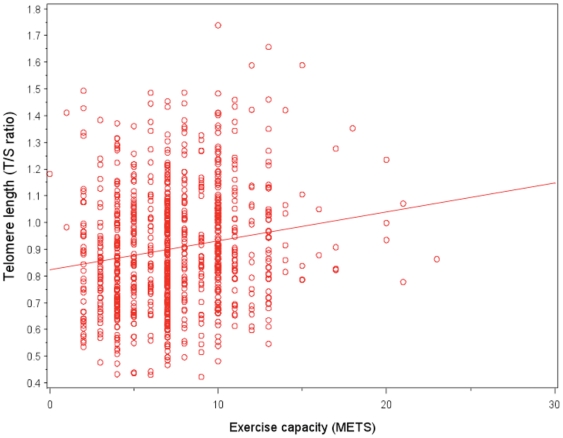
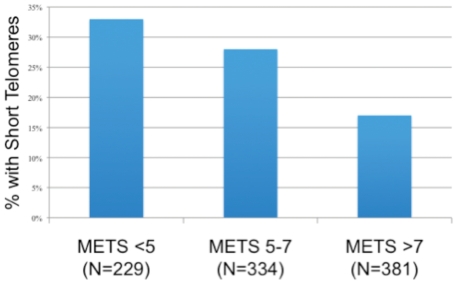
In a cross sectional study of 944 outpatients with stable CHD, we performed exercise treadmill testing, assessed self-reported physical activity, and measured leukocyte TL using a quantitative PCR assay. We used generalized linear models to calculate mean TL (T/S ratio), and logistic regression models to compare the proportion of patients with short TL (defined as the lowest quartile), among participants with low, medium and high physical fitness, based on metabolic equivalent tasks achieved (METs).
229 participants had low physical fitness (<5 METS), 334 had moderate physical fitness (5-7 METS), and 381 had high physical fitness (>7 METS). Mean ± T/S ratio ranged from 0.86±0.21 (5349±3781 base pairs) in those with low physical fitness to 0.95±0.23 (5566±3829 base pairs) in those with high physical fitness (p<.001). This association remained strong after adjustment for numerous patient characteristics, including measures of cardiac disease severity and physical inactivity (p = 0.005). Compared with participants with high physical fitness, those with low physical fitness had 2-fold greater odds of having TL in the lowest quartile (OR 2.39, 95% CI 1.60-3.55; p<.001). This association was similar after multivariable adjustment (OR 1.94, 95%CI, 1.18-3.20; p = 0.009). Self-reported physical inactivity was associated with shorter TL in unadjusted analyses, but not after multivariable adjustment.
We found that worse objectively-assessed physical fitness is associated with shorter leukocyte telomere length in patients with CHD. The clinical implications of this association deserve further study.
端粒长度较短(TL)是冠心病(CHD)患者死亡的独立预测因素。然而,在这些患者中,身体状况与 TL 之间的关系尚未得到探索。
在一项对 944 名稳定型 CHD 门诊患者的横断面研究中,我们进行了运动平板测试,评估了自我报告的体力活动,并使用定量 PCR 检测白细胞 TL。我们使用广义线性模型计算平均 TL(T/S 比值),并使用逻辑回归模型比较了根据代谢当量任务(MET)获得的低、中、高体力活动组中 TL 较短(定义为最低四分位数)的患者比例。
229 名患者体力活动较差(<5 MET),334 名患者体力活动中等(5-7 MET),381 名患者体力活动较好(>7 MET)。平均 T/S 比值范围从体力活动较差的患者(0.86±0.21,5349±3781 个碱基对)到体力活动较好的患者(0.95±0.23,5566±3829 个碱基对)(p<.001)。在调整了许多患者特征,包括心脏病严重程度和体力活动不足的测量值后,这种关联仍然很强(p=0.005)。与体力活动较好的患者相比,体力活动较差的患者 TL 处于最低四分位数的可能性高 2 倍(OR 2.39,95%CI 1.60-3.55;p<.001)。多变量调整后,这种关联相似(OR 1.94,95%CI,1.18-3.20;p=0.009)。未调整分析中,自我报告的体力活动不足与较短的 TL 相关,但多变量调整后则不然。
我们发现,在 CHD 患者中,较差的客观评估身体状况与白细胞端粒长度较短有关。这种关联的临床意义值得进一步研究。