Epidemiology and Global Health, Department of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden.
Cost Eff Resour Alloc. 2011 Nov 18;9(1):17. doi: 10.1186/1478-7547-9-17.
Type 2 diabetes mellitus (T2D) poses a large worldwide burden for health care systems. One possible tool to decrease this burden is primary prevention. As it is unethical to wait until perfect data are available to conclude whether T2D primary prevention intervention programmes are cost-effective, we need a model that simulates the effect of prevention initiatives. Thus, the aim of this study is to investigate the long-term cost-effectiveness of lifestyle intervention programmes for the prevention of T2D using a Markov model. As decision makers often face difficulties in applying health economic results, we visualise our results with health economic tools.
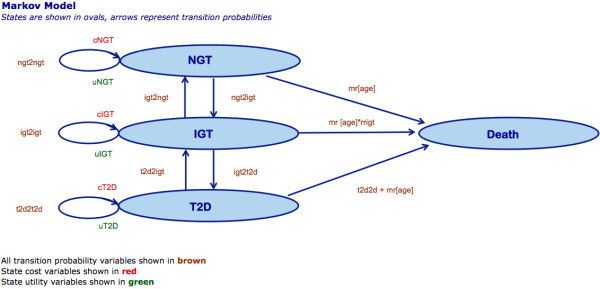
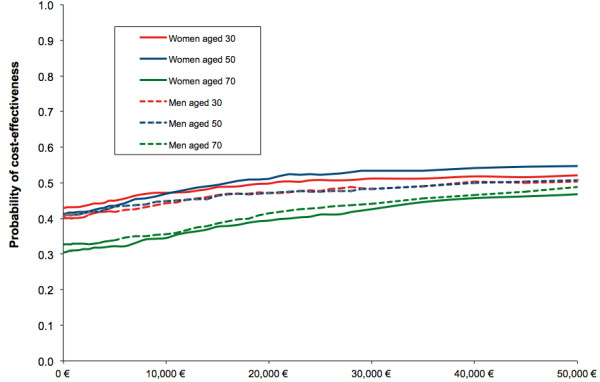
We use four-state Markov modelling with a probabilistic cohort analysis to calculate the cost per quality-adjusted life year (QALY) gained. A one-year cycle length and a lifetime time horizon are applied. Best available evidence supplies the model with data on transition probabilities between glycaemic states, mortality risks, utility weights, and disease costs. The costs are calculated from a societal perspective. A 3% discount rate is used for costs and QALYs. Cost-effectiveness acceptability curves are presented to assist decision makers.
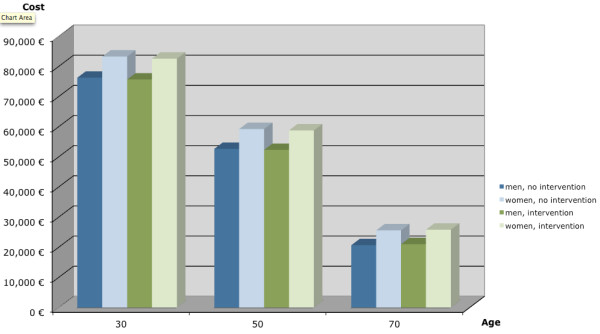
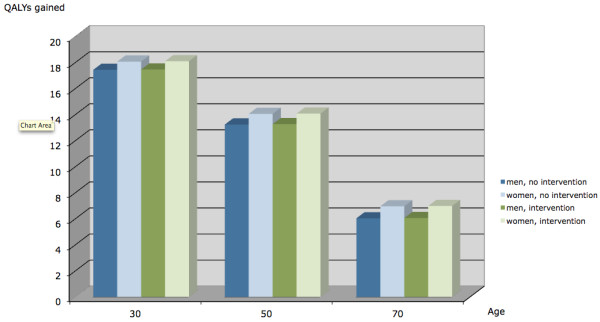
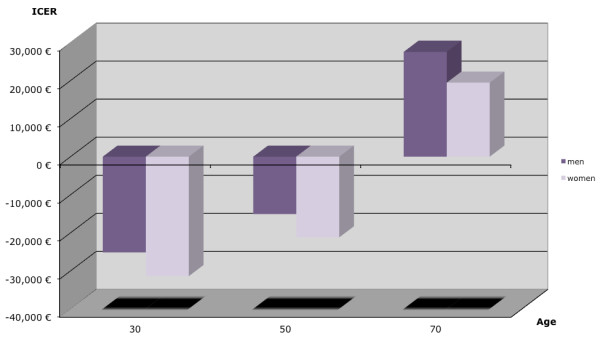
The model indicates that diabetes prevention interventions have the potential to be cost-effective, but the outcome reveals a high level of uncertainty. Incremental cost-effectiveness ratios (ICERs) were negative for the intervention, ie, the intervention leads to a cost reduction for men and women aged 30 or 50 years at initiation of the intervention. For men and women aged 70 at initiation of the intervention, the ICER was EUR27,546/QALY gained and EUR19,433/QALY gained, respectively. In all cases, the QALYs gained were low. Cost-effectiveness acceptability curves show that the higher the willingness-to-pay threshold value, the higher the probability that the intervention is cost-effective. Nonetheless, all curves are flat. The threshold value of EUR50,000/QALY gained has a 30-55% probability that the intervention is cost-effective.
Lifestyle interventions for primary prevention of type 2 diabetes are cost-saving for men and women aged 30 or 50 years at the start of the intervention, and cost-effective for men and women aged 70 years. However, there is a high degree of uncertainty around the ICERs. With the conservative approach adopted for this model, the long-term effectiveness of the intervention could be underestimated.
2 型糖尿病(T2D)给全球医疗系统带来了巨大负担。降低这种负担的一种可能方法是初级预防。由于在等待获得完美数据以确定 T2D 初级预防干预计划是否具有成本效益方面是不道德的,因此我们需要一种能够模拟预防措施效果的模型。因此,本研究旨在使用马尔可夫模型研究生活方式干预预防 T2D 的长期成本效益。由于决策者在应用健康经济学结果时经常面临困难,因此我们使用健康经济学工具来可视化我们的结果。
我们使用具有概率队列分析的四状态马尔可夫模型来计算每获得一个质量调整生命年(QALY)的成本。采用一年的周期长度和终生的时间范围。最佳可用证据为模型提供了关于血糖状态之间的转移概率、死亡率风险、效用权重和疾病成本的数据。成本是从社会角度计算的。使用 3%的贴现率计算成本和 QALY。呈现成本效益接受曲线以帮助决策者。
该模型表明,糖尿病预防干预有可能具有成本效益,但结果显示存在高度的不确定性。对于男性和女性,当他们在干预开始时分别为 30 岁或 50 岁时,干预的增量成本效益比(ICER)为负值,即干预导致成本降低。对于在干预开始时年龄为 70 岁的男性和女性,ICER 分别为 27546 欧元/QALY 获得和 19433 欧元/QALY 获得。在所有情况下,获得的 QALY 都很低。成本效益接受曲线表明,支付意愿阈值越高,干预具有成本效益的可能性就越高。尽管如此,所有曲线都是平坦的。在 50000 欧元/QALY 获得的阈值下,干预具有成本效益的概率为 30-55%。
对于在干预开始时分别为 30 岁或 50 岁的男性和女性,生活方式干预进行 T2D 的初级预防是节省成本的,对于在干预开始时年龄为 70 岁的男性和女性,干预是具有成本效益的。然而,ICER 存在高度的不确定性。由于该模型采用了保守的方法,干预的长期效果可能被低估了。