Department Child Health, TNO Netherlands Organization for Applied Scientific Research, Leiden, The Netherlands.
PLoS One. 2011;6(11):e24727. doi: 10.1371/journal.pone.0024727. Epub 2011 Nov 16.
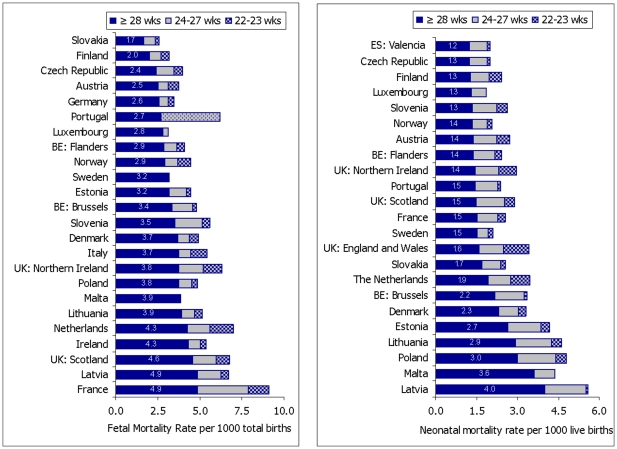
The first European Perinatal Health Report showed wide variability between European countries in fetal (2.6-9.1‰) and neonatal (1.6-5.7‰) mortality rates in 2004. We investigated gestational age patterns of fetal and neonatal mortality to improve our understanding of the differences between countries with low and high mortality.
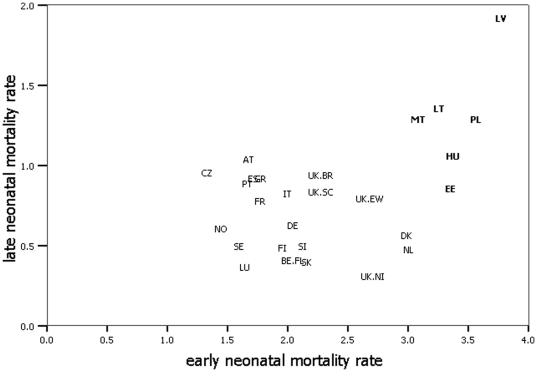
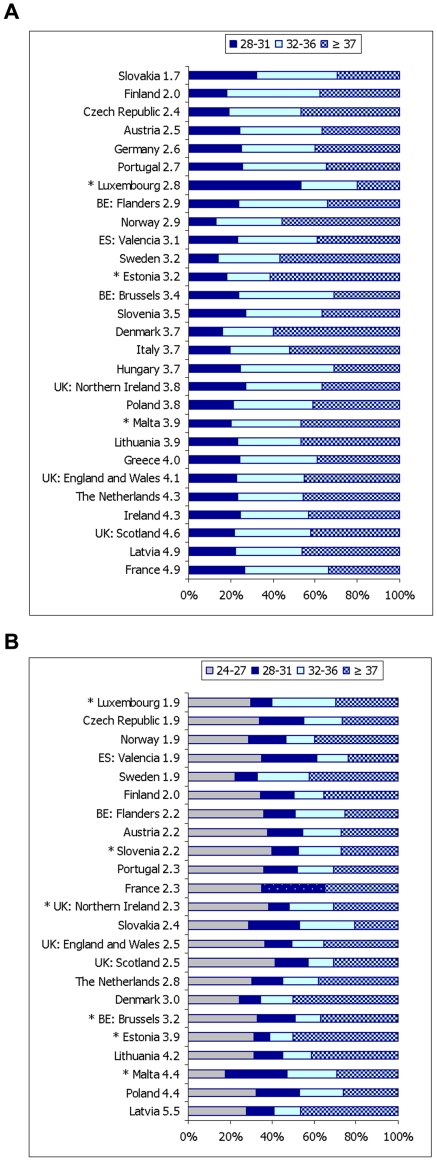
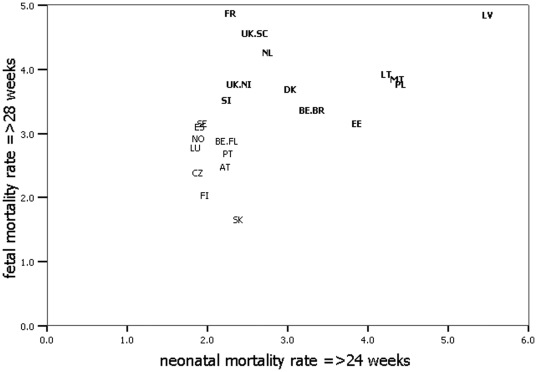
METHODOLOGY/PRINCIPAL FINDINGS: Data on 29 countries/regions participating in the Euro-Peristat project were analyzed. Most European countries had no limits for the registration of live births, but substantial variations in limits for registration of stillbirths before 28 weeks of gestation existed. Country rankings changed markedly after excluding deaths most likely to be affected by registration differences (22-23 weeks for neonatal mortality and 22-27 weeks for fetal mortality). Countries with high fetal mortality ≥28 weeks had on average higher proportions of fetal deaths at and near term (≥37 weeks), while proportions of fetal deaths at earlier gestational ages (28-31 and 32-36 weeks) were higher in low fetal mortality countries. Countries with high neonatal mortality rates ≥24 weeks, all new member states of the European Union, had high gestational age-specific neonatal mortality rates for all gestational-age subgroups; they also had high fetal mortality, as well as high early and late neonatal mortality. In contrast, other countries with similar levels of neonatal mortality had varying levels of fetal mortality, and among these countries early and late neonatal mortality were negatively correlated.
For valid European comparisons, all countries should register births and deaths from at least 22 weeks of gestation and should be able to distinguish late terminations of pregnancy from stillbirths. After excluding deaths most likely to be influenced by existing registration differences, important variations in both levels and patterns of fetal and neonatal mortality rates were found. These disparities raise questions for future research about the effectiveness of medical policies and care in European countries.
《第一份欧洲围产保健报告》显示,2004 年欧洲各国的胎儿(2.6-9.1‰)和新生儿(1.6-5.7‰)死亡率存在较大差异。为了深入了解高死亡率和低死亡率国家之间的差异,我们研究了胎儿和新生儿死亡率的胎龄模式。
方法/主要发现:对参与 Euro-Peristat 项目的 29 个国家/地区的数据进行了分析。大多数欧洲国家对活产的登记没有限制,但 28 周前死产的登记限制存在很大差异。在排除了可能受登记差异影响的死亡(新生儿死亡率为 22-23 周,胎儿死亡率为 22-27 周)后,国家排名发生了显著变化。28 周以上胎儿死亡率较高的国家,平均而言,接近足月(≥37 周)的胎儿死亡比例较高,而 28-31 周和 32-36 周的胎儿死亡比例在低胎儿死亡率国家较高。24 周以上新生儿死亡率较高的国家(均为新加入欧盟的成员国),所有胎龄组的特定胎龄新生儿死亡率均较高;它们也有较高的胎儿死亡率,以及较高的早期和晚期新生儿死亡率。相比之下,其他具有类似新生儿死亡率水平的国家则有不同程度的胎儿死亡率,而在这些国家中,早期和晚期新生儿死亡率呈负相关。
为了进行有效的欧洲比较,所有国家都应至少从 22 周开始登记分娩和死亡,并能够区分晚期妊娠终止和死产。在排除了可能受到现有登记差异影响的死亡后,发现胎儿和新生儿死亡率的水平和模式存在重要差异。这些差异引发了关于欧洲国家医疗政策和护理有效性的未来研究问题。