National Resource Center for Rehabilitation in Rheumatology, Diakonhjemmet Hospital, PO Box 23 Vinderen, No-0319 Oslo, Norway.
Arthritis Res Ther. 2012 Jan 25;14(1):R19. doi: 10.1186/ar3699.
Pulmonary involvement is a known manifestation in patients with ankylosing spondylitis (AS). However, previous studies have been based on small samples and the reported prevalence and associations with typical clinical features vary. The purpose of this study was to compare pulmonary function (PF) in patients with AS and population controls, and to study associations between PF and disease related variables, cardio-respiratory fitness and demographic variables in patients with AS.
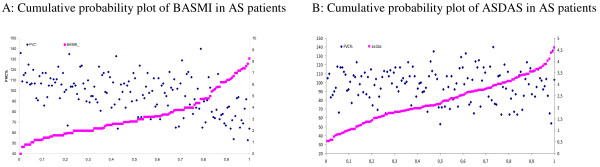
In a cross-sectional controlled study, 147 AS patients and 121 controls underwent examinations, including demographic variables, laboratory (C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)) and clinical measures (disease activity (AS disease activity score, ASDAS), physical function (Bath ankylosing spondylitis functional index, BASFI), spinal mobility (Bath ankylosing spondylitis metrology index, BASMI), chest expansion, cardio-respiratory fitness (peak oxygen uptake, VO(2peak) and pulmonary function test (PFT) (spirometry)). Cumulative probability plots were used to visualize associations between the ASDAS and BASMI scores and the corresponding forced vital capacity (FVC%, percentage of predicted value controlled for the influence of confounding factors) score for each patient. Univariate ANCOVAs were performed to explore group differences in PF adjusting for relevant variables, and a multiple regression model was used to estimate the explanatory power of independent variables (demographic, disease related, VO(2peak) on restrictive ventilatory impairment (FVC%).
AS patients showed significantly lower PF values compared with controls, and significantly more patients were categorized with restrictive pattern (18% vs. 0%, P < 0.001). Cumulative probability plots showed significant associations between spinal mobility measures (BASMI) and FVC% for individual patients. BASMI, chest expansion and male gender contributed significantly and independently in a multiple regression model predicting the variation of FVC% in AS patients, whereas disease activity, physical function and VO(2peak) did not contribute significantly. The final model explained 45% of the variance in FVC% (P < 0.001).
This study showed significantly impaired pulmonary function in the AS patients compared to controls and reference data, and demonstrated a clear relationship between reduced spinal mobility and restrictive PF in AS patients. The results support the assumption of an association between musculoskeletal limitations and restrictive respiratory impairment in AS, emphasizing the importance of maintaining spinal flexibility in the management of the disease. Further, patients with severely reduced spinal mobility should be referred for pulmonary function examination and relevant follow-up treatment.
肺脏受累是强直性脊柱炎(AS)患者的一种已知表现。然而,以前的研究基于小样本,报道的患病率和与典型临床特征的相关性各不相同。本研究的目的是比较 AS 患者和人群对照的肺功能(PF),并研究 PF 与疾病相关变量、心肺功能和 AS 患者的人口统计学变量之间的相关性。
在一项横断面对照研究中,147 例 AS 患者和 121 例对照接受了检查,包括人口统计学变量、实验室(C 反应蛋白(CRP)、红细胞沉降率(ESR))和临床指标(疾病活动度(AS 疾病活动评分,ASDAS)、身体功能(巴斯强直性脊柱炎功能指数,BASFI)、脊柱活动度(巴斯强直性脊柱炎计量指数,BASMI)、胸廓扩张、心肺功能(峰值摄氧量,VO₂peak)和肺功能检查(肺活量测定法)(肺量计))。累积概率图用于可视化 ASDAS 和 BASMI 评分与每个患者相应的用力肺活量(FVC%,受混杂因素影响的预测值校正)评分之间的关系。进行单变量协方差分析,以调整相关变量后比较 PF 的组间差异,并使用多元回归模型估计独立变量(人口统计学、疾病相关、VO₂peak)对限制性通气障碍(FVC%)的解释能力。
与对照组相比,AS 患者的 PF 值明显较低,且明显更多的患者被归类为限制性模式(18%对 0%,P < 0.001)。累积概率图显示脊柱活动度指标(BASMI)与个体患者的 FVC%之间存在显著关联。在预测 AS 患者 FVC%变化的多元回归模型中,BASMI、胸廓扩张和男性性别具有显著且独立的贡献,而疾病活动度、身体功能和 VO₂peak 则没有显著贡献。最终模型解释了 FVC%变异的 45%(P < 0.001)。
本研究显示,与对照组和参考数据相比,AS 患者的肺功能明显受损,并显示出 AS 患者脊柱活动度降低与限制性 PF 之间的明确关系。结果支持肌肉骨骼受限与 AS 中限制性呼吸损害之间存在关联的假设,强调了在疾病管理中保持脊柱灵活性的重要性。此外,脊柱活动度严重降低的患者应转介进行肺功能检查和相关随访治疗。