Department of Radiology, University of Tokyo Hospital, Hongo, Bunkyo-ku, Tokyo, Japan.
Radiat Oncol. 2012 Feb 9;7:20. doi: 10.1186/1748-717X-7-20.
The purpose of this study was to compare dose distributions from three different algorithms with the x-ray Voxel Monte Carlo (XVMC) calculations, in actual computed tomography (CT) scans for use in stereotactic radiotherapy (SRT) of small lung cancers.
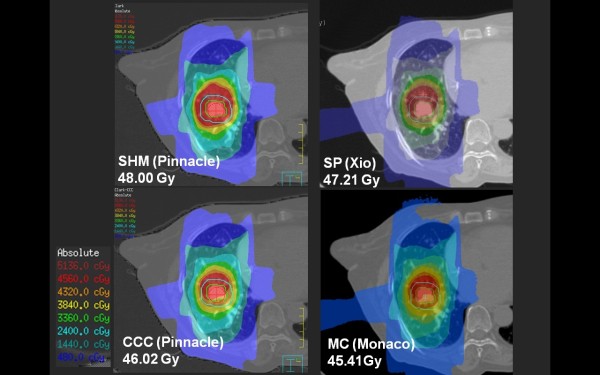
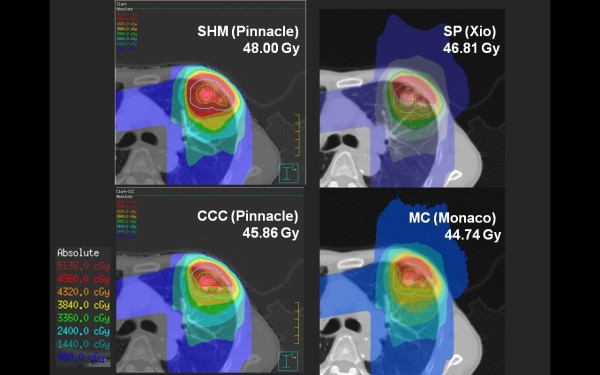
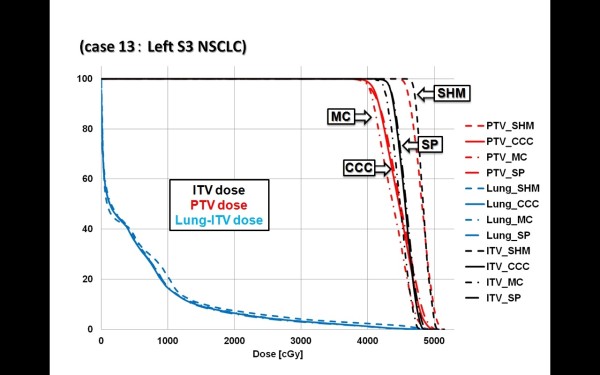
Slow CT scan of 20 patients was performed and the internal target volume (ITV) was delineated on Pinnacle3. All plans were first calculated with a scatter homogeneous mode (SHM) which is compatible with Clarkson algorithm using Pinnacle3 treatment planning system (TPS). The planned dose was 48 Gy in 4 fractions. In a second step, the CT images, structures and beam data were exported to other treatment planning systems (TPSs). Collapsed cone convolution (CCC) from Pinnacle3, superposition (SP) from XiO, and XVMC from Monaco were used for recalculating. The dose distributions and the Dose Volume Histograms (DVHs) were compared with each other.
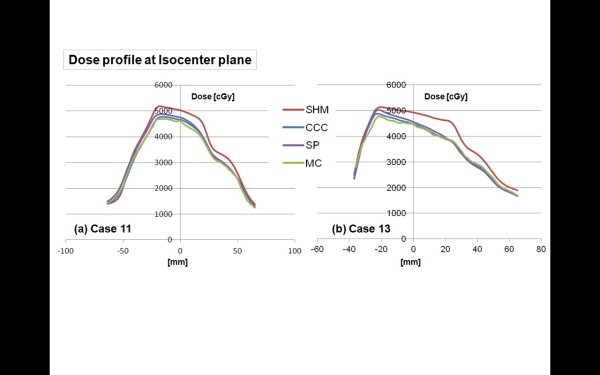
The phantom test revealed that all algorithms could reproduce the measured data within 1% except for the SHM with inhomogeneous phantom. For the patient study, the SHM greatly overestimated the isocenter (IC) doses and the minimal dose received by 95% of the PTV (PTV95) compared to XVMC. The differences in mean doses were 2.96 Gy (6.17%) for IC and 5.02 Gy (11.18%) for PTV95. The DVH's and dose distributions with CCC and SP were in agreement with those obtained by XVMC. The average differences in IC doses between CCC and XVMC, and SP and XVMC were -1.14% (p = 0.17), and -2.67% (p = 0.0036), respectively.
Our work clearly confirms that the actual practice of relying solely on a Clarkson algorithm may be inappropriate for SRT planning. Meanwhile, CCC and SP were close to XVMC simulations and actual dose distributions obtained in lung SRT.
本研究旨在比较三种不同算法与 X 射线体素蒙特卡罗(XVMC)计算的剂量分布,这些算法应用于小肺癌立体定向放疗(SRT)的实际计算机断层扫描(CT)扫描中。
对 20 名患者进行慢速 CT 扫描,并在 Pinnacle3 上勾画内部靶区(ITV)。所有计划均首先使用与 Clarkson 算法兼容的散射均匀模式(SHM)在 Pinnacle3 治疗计划系统(TPS)中进行计算。计划剂量为 48Gy,分为 4 个部分。在第二步中,将 CT 图像、结构和射束数据导出到其他治疗计划系统(TPS)。使用 Pinnacle3 的锥形束卷积(CCC)、XiO 的叠加(SP)和 Monaco 的 XVMC 进行重新计算。比较剂量分布和剂量体积直方图(DVH)。
除了不均匀体模的 SHM 外,所有算法都可以在 1%以内重现测量数据。对于患者研究,与 XVMC 相比,SHM 大大高估了等中心(IC)剂量和 95%的 PTV(PTV95)接受的最小剂量。IC 平均剂量的差异为 2.96Gy(6.17%),PTV95 为 5.02Gy(11.18%)。CCC 和 SP 的 DVH 和剂量分布与 XVMC 一致。CCC 与 XVMC 和 SP 与 XVMC 的 IC 剂量平均差异分别为-1.14%(p=0.17)和-2.67%(p=0.0036)。
我们的工作清楚地证实,仅依靠 Clarkson 算法的实际做法可能不适合 SRT 计划。同时,CCC 和 SP 与 XVMC 模拟和肺 SRT 中实际获得的剂量分布非常接近。