Department of Psychiatry, Herchel Smith Building for Brain and Mind Sciences, University of Cambridge, Cambridge, United Kingdom.
PLoS One. 2012;7(3):e31660. doi: 10.1371/journal.pone.0031660. Epub 2012 Mar 22.
We conducted a systematic review of incidence rates in England over a sixty-year period to determine the extent to which rates varied along accepted (age, sex) and less-accepted epidemiological gradients (ethnicity, migration and place of birth and upbringing, time).
To determine variation in incidence of several psychotic disorders as above.
Published and grey literature searches (MEDLINE, PSycINFO, EMBASE, CINAHL, ASSIA, HMIC), and identification of unpublished data through bibliographic searches and author communication.
Published 1950-2009; conducted wholly or partially in England; original data on incidence of non-organic adult-onset psychosis or one or more factor(s) pertaining to incidence.
People, 16-64 years, with first -onset psychosis, including non-affective psychoses, schizophrenia, bipolar disorder, psychotic depression and substance-induced psychosis.
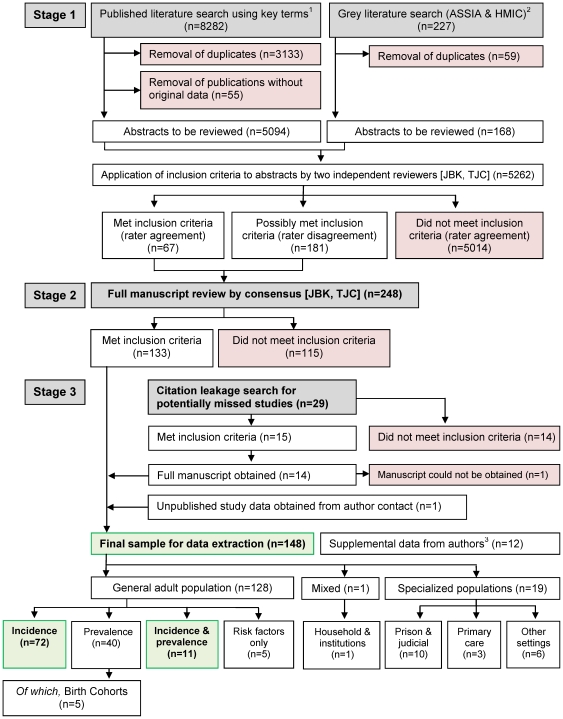
Title, abstract and full-text review by two independent raters to identify suitable citations. Data were extracted to a standardized extraction form. Descriptive appraisals of variation in rates, including tables and forest plots, and where suitable, random-effects meta-analyses and meta-regressions to test specific hypotheses; rate heterogeneity was assessed by the I²-statistic.
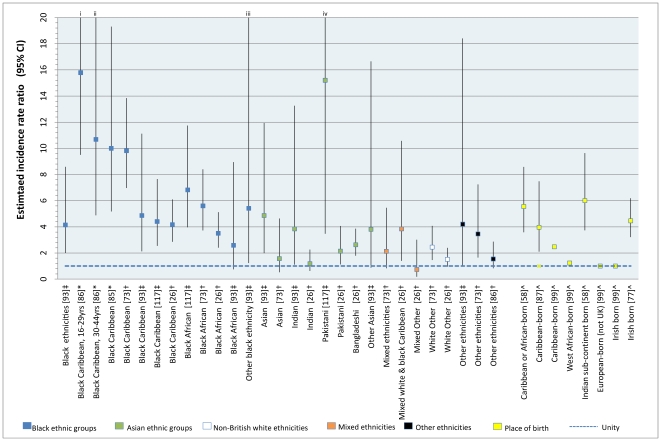
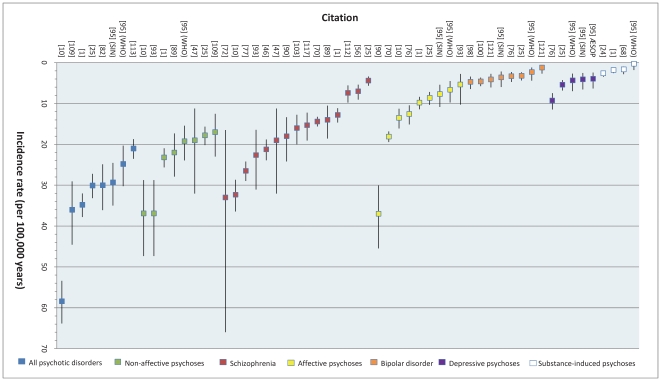
83 citations met inclusion. Pooled incidence of all psychoses (N = 9) was 31.7 per 100,000 person-years (95%CI: 24.6-40.9), 23.2 (95%CI: 18.3-29.5) for non-affective psychoses (N = 8), 15.2 (95%CI: 11.9-19.5) for schizophrenia (N = 15) and 12.4 (95%CI: 9.0-17.1) for affective psychoses (N = 7). This masked rate heterogeneity (I²: 0.54-0.97), possibly explained by socio-environmental factors; our review confirmed (via meta-regression) the typical age-sex interaction in psychosis risk, including secondary peak onset in women after 45 years. Rates of most disorders were elevated in several ethnic minority groups compared with the white (British) population. For example, for schizophrenia: black Caribbean (pooled RR: 5.6; 95%CI: 3.4-9.2; N = 5), black African (pooled RR: 4.7; 95%CI: 3.3-6.8; N = 5) and South Asian groups in England (pooled RR: 2.4; 95%CI: 1.3-4.5; N = 3). We found no evidence to support an overall change in the incidence of psychotic disorder over time, though diagnostic shifts (away from schizophrenia) were reported.
Incidence studies were predominantly cross-sectional, limiting causal inference. Heterogeneity, while evidencing important variation, suggested pooled estimates require interpretation alongside our descriptive systematic results.
Incidence of psychotic disorders varied markedly by age, sex, place and migration status/ethnicity. Stable incidence over time, together with a robust socio-environmental epidemiology, provides a platform for developing prediction models for health service planning.
我们对英格兰 60 年来的发病率进行了系统回顾,以确定在多大程度上接受的(年龄、性别)和不太接受的(种族、移民以及出生地和成长地、时间)流行病学梯度上存在差异。
确定上述几种精神病发病率的变化情况。
通过 MEDLINE、PSycINFO、EMBASE、CINAHL、ASSIA、HMIC 进行了已发表和灰色文献检索,并通过文献检索和作者沟通确定了未发表的数据。
发表于 1950 年至 2009 年;在英格兰进行的全部或部分研究;有关于非器质性成人发病精神病或与发病相关的一个或多个因素的原始数据。
年龄在 16-64 岁之间的首次发病的成年人,包括非情感性精神病、精神分裂症、双相情感障碍、精神病性抑郁症和物质引起的精神病。
两名独立评审员对标题、摘要和全文进行审查,以确定合适的文献。将数据提取到标准化的提取表格中。使用表格和森林图对发病率的变化进行描述性评估,并在适当的情况下进行随机效应荟萃分析和荟萃回归以检验特定假设;使用 I² 统计量评估率异质性。
有 83 篇文献符合纳入标准。所有精神病的合并发病率(N=9)为 31.7/100,000 人年(95%CI:24.6-40.9),非情感性精神病的发病率(N=8)为 23.2(95%CI:18.3-29.5),精神分裂症的发病率(N=15)为 15.2(95%CI:11.9-19.5),情感性精神病的发病率(N=7)为 12.4(95%CI:9.0-17.1)。这掩盖了发病率的异质性(I²:0.54-0.97),可能与社会环境因素有关;我们的综述通过荟萃回归证实了精神病风险中的典型年龄性别相互作用,包括女性在 45 岁以后的第二个发病高峰。与白种人(英国)相比,许多种族群体的精神病发病率较高。例如,对于精神分裂症:加勒比黑人(RR:5.6;95%CI:3.4-9.2;N=5)、非洲黑人(RR:4.7;95%CI:3.3-6.8;N=5)和英国的南亚群体(RR:2.4;95%CI:1.3-4.5;N=3)。我们没有发现任何证据表明精神病发病率随时间发生变化,尽管有报道称诊断发生了转变(远离精神分裂症)。
发病率研究主要是横断面研究,限制了因果推断。虽然异质性表明,汇总估计值需要与我们的描述性系统结果一起解释,但它也证明了存在重要的差异。
精神病发病率在年龄、性别、地点和移民状况/种族方面存在显著差异。随着时间的推移,发病率保持稳定,再加上稳健的社会环境流行病学,为制定卫生服务规划的预测模型提供了一个平台。