National Institute for Occupational Safety and Health, Health Effects Laboratory Division, Morgantown, West Virginia, USA.
J Occup Environ Hyg. 2012;9(7):443-9. doi: 10.1080/15459624.2012.684582.
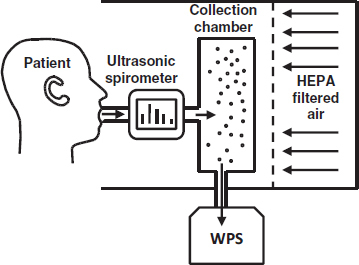
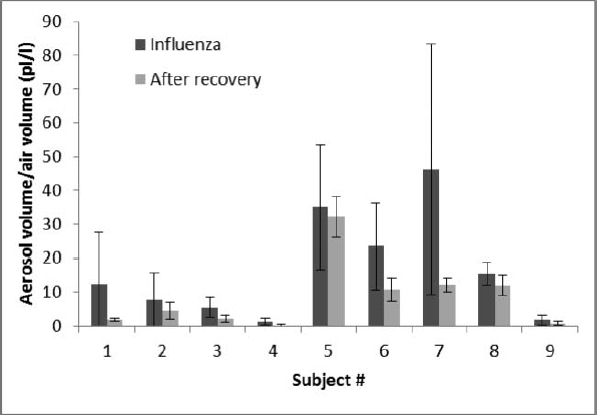
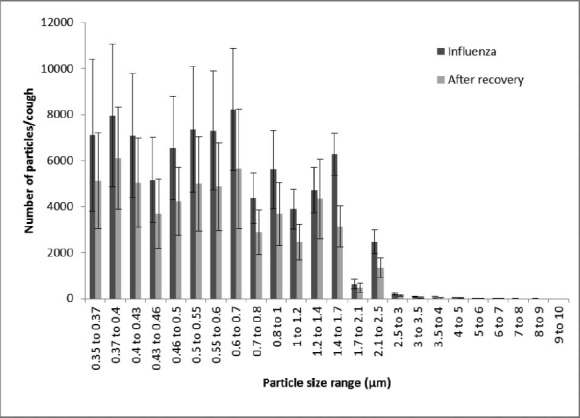
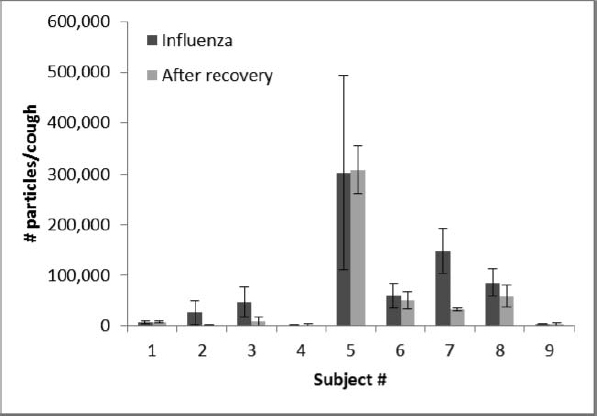
The question of whether influenza is transmitted to a significant degree by aerosols remains controversial, in part, because little is known about the quantity and size of potentially infectious airborne particles produced by people with influenza. In this study, the size and amount of aerosol particles produced by nine subjects during coughing were measured while they had influenza and after they had recovered, using a laser aerosol particle spectrometer with a size range of 0.35 to 10 μm. Individuals with influenza produce a significantly greater volume of aerosol when ill compared with afterward (p = 0.0143). When the patients had influenza, their average cough aerosol volume was 38.3 picoliters (pL) of particles per cough (SD 43.7); after patients recovered, the average volume was 26.4 pL per cough (SD 45.6). The number of particles produced per cough was also higher when subjects had influenza (average 75,400 particles/cough, SD 97,300) compared with afterward (average 52,200, SD 98,600), although the difference did not reach statistical significance (p = 0.1042). The average number of particles expelled per cough varied widely from patient to patient, ranging from 900 to 302,200 particles/cough while subjects had influenza and 1100 to 308,600 particles/cough after recovery. When the subjects had influenza, an average of 63% of each subject's cough aerosol particle volume in the detection range was in the respirable size fraction (SD 22%), indicating that these particles could reach the alveolar region of the lungs if inhaled by another person. This enhancement in aerosol generation during illness may play an important role in influenza transmission and suggests that a better understanding of this phenomenon is needed to predict the production and dissemination of influenza-laden aerosols by people infected with this virus. [Supplementary materials are available for this article. Go to the publisher's online edition of Journal of Occupational and Environmental Hygiene for the following free supplemental resources: a PDF file of demographic information, influenza test results, and volume and peak flow rate during each cough and a PDF file containing number and size of aerosol particles produced.].
关于流感是否在很大程度上通过气溶胶传播,这一问题仍然存在争议,部分原因是人们对流感患者产生的具有潜在传染性的空气传播飞沫的数量和大小知之甚少。在这项研究中,使用激光气溶胶粒子谱仪(粒径范围为 0.35 至 10μm),对 9 名流感患者咳嗽时产生的气溶胶粒子的大小和数量进行了测量,这 9 名患者在患病和康复后分别进行了测量。与康复后相比,流感患者咳嗽时产生的气溶胶体积明显更大(p = 0.0143)。当患者患有流感时,他们每次咳嗽的平均咳嗽气溶胶体积为 38.3 皮升(pL)的颗粒(SD 43.7);在患者康复后,每次咳嗽的平均体积为 26.4 pL(SD 45.6)。与康复后相比,患者咳嗽时产生的颗粒数量也更高(平均每咳嗽 75400 个颗粒/咳嗽,SD 97300),尽管差异没有达到统计学意义(p = 0.1042)。每个患者每次咳嗽排出的颗粒数量差异很大,范围从 900 到 302200 个颗粒/咳嗽,而在患者患病时,范围从 1100 到 308600 个颗粒/咳嗽。当患者患有流感时,每个患者咳嗽气溶胶粒子体积的检测范围内的平均有 63%是可吸入的粒径部分(SD 22%),这表明如果另一个人吸入这些颗粒,它们可能会到达肺部的肺泡区域。在患病期间,气溶胶生成的这种增强可能在流感传播中发挥重要作用,这表明需要更好地了解这种现象,以便预测感染这种病毒的人产生和传播携带流感病毒的气溶胶。[本文提供了补充材料。请访问《职业与环境卫生杂志》的出版商在线版本,获取以下免费补充资源:一份 PDF 文件,其中包含人口统计学信息、流感检测结果以及每次咳嗽的体积和峰值流量;以及一份包含产生的气溶胶粒子数量和大小的 PDF 文件。]