Centre for Infectious Diseases and Microbiology, Westmead Hospital, Sydney, New South Wales, Australia.
PLoS One. 2012;7(6):e38719. doi: 10.1371/journal.pone.0038719. Epub 2012 Jun 25.
Antibiotic homogeneity is thought to drive resistance but in vivo data are lacking. In this study, we determined the impact of antibiotic homogeneity per se, and of cefepime versus antipseudomonal penicillin/β-lactamase inhibitor combinations (APP-β), on the likelihood of infection or colonisation with antibiotic resistant bacteria and/or two commonly resistant nosocomial pathogens (methicillin-resistant Staphylococcus aureus and Pseudomonas aeruginosa). A secondary question was whether antibiotic cycling was associated with adverse outcomes including mortality, length of stay, and antibiotic resistance.
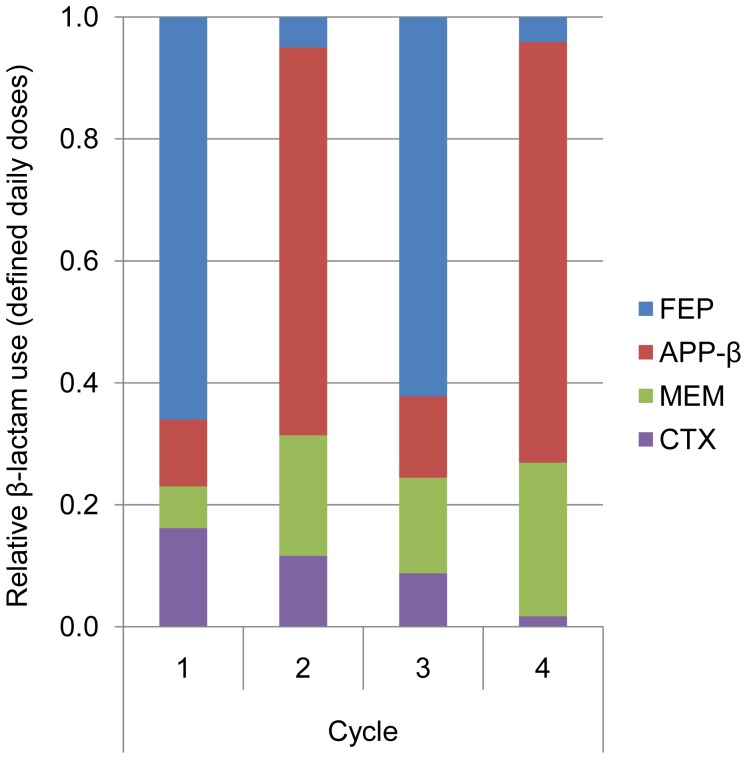
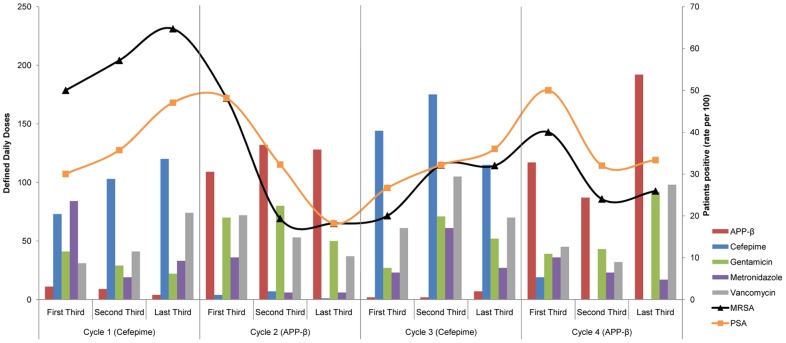
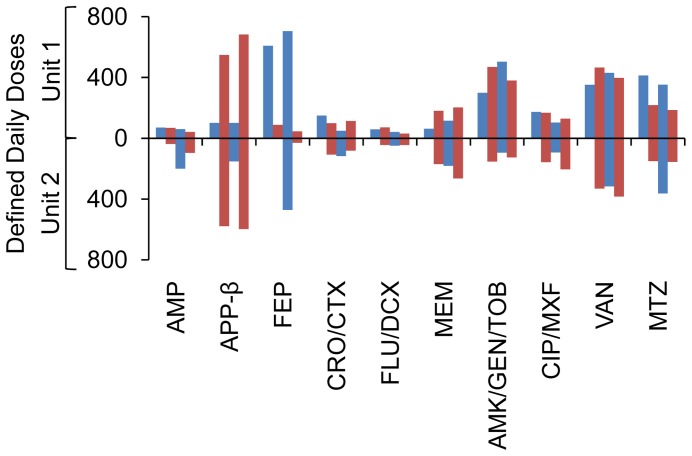
We evaluated clinical and microbiological outcomes in two similar metropolitan ICUs, which both alternated cefepime with APP-β in four-month cycles. All microbiological isolates and commensal samples were analysed for the presence of antibiotic-resistant bacteria including MRSA and P. aeruginosa.
Length of stay, mortality and overall antibiotic resistance were unchanged after sixteen months. However, increased colonisation and infection by antibiotic-resistant bacteria were observed in cefepime cycles, returning to baseline in APP-β cycles. Cefepime was the strongest risk factor for acquisition of antibiotic-resistant infection.
Ecological effects of different β-lactam antibiotics may be more important than specific activity against the causative agents or the effect of antibiotic homogeneity in selection for antibiotic resistance. This has important implications for antibiotic policy.
抗生素同质化被认为会导致耐药性,但体内数据缺乏。在这项研究中,我们确定了抗生素同质化本身,以及头孢吡肟与抗假单胞菌青霉素/β-内酰胺酶抑制剂联合制剂(APP-β)对感染或定植耐药菌和/或两种常见耐药医院病原体(耐甲氧西林金黄色葡萄球菌和铜绿假单胞菌)的可能性的影响。第二个问题是抗生素轮替是否与不良结局相关,包括死亡率、住院时间和抗生素耐药性。
我们评估了两个类似的大都市 ICU 的临床和微生物学结局,这两个 ICU 均以四个月为一个周期交替使用头孢吡肟和 APP-β。所有微生物分离株和共生样本均分析了包括耐甲氧西林金黄色葡萄球菌和铜绿假单胞菌在内的耐药菌的存在情况。
在十六个月后,住院时间、死亡率和总体抗生素耐药性没有变化。然而,在头孢吡肟周期中观察到耐药菌的定植和感染增加,在 APP-β 周期中恢复到基线。头孢吡肟是获得耐药性感染的最强危险因素。
不同β-内酰胺类抗生素的生态效应可能比针对病原体的特定活性或抗生素同质化对耐药性选择的影响更重要。这对抗生素政策具有重要意义。