Wang Lu, Rotnitzky Andrea, Lin Xihong, Millikan Randall E, Thall Peter F
Department of Biostatistics, University of Michigan, Ann Arbor, MI 48109.
J Am Stat Assoc. 2012 Jun;107(498):493-508. doi: 10.1080/01621459.2011.641416.
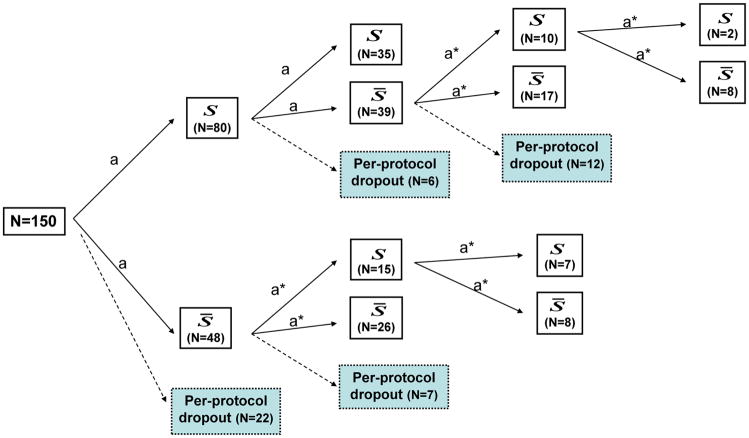
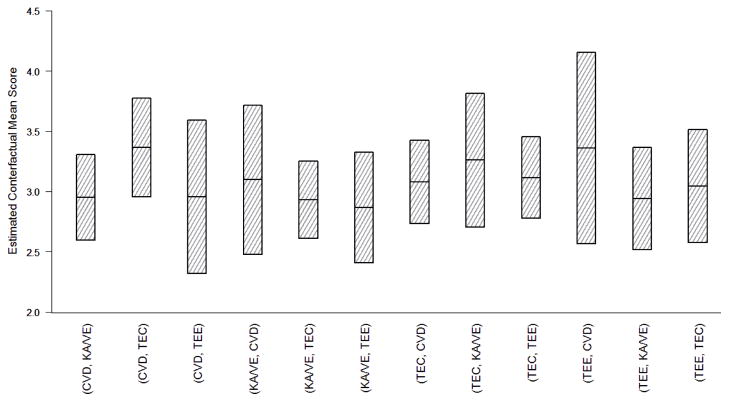
We present new statistical analyses of data arising from a clinical trial designed to compare two-stage dynamic treatment regimes (DTRs) for advanced prostate cancer. The trial protocol mandated that patients were to be initially randomized among four chemotherapies, and that those who responded poorly were to be rerandomized to one of the remaining candidate therapies. The primary aim was to compare the DTRs' overall success rates, with success defined by the occurrence of successful responses in each of two consecutive courses of the patient's therapy. Of the one hundred and fifty study participants, forty seven did not complete their therapy per the algorithm. However, thirty five of them did so for reasons that precluded further chemotherapy; i.e. toxicity and/or progressive disease. Consequently, rather than comparing the overall success rates of the DTRs in the unrealistic event that these patients had remained on their assigned chemotherapies, we conducted an analysis that compared viable switch rules defined by the per-protocol rules but with the additional provision that patients who developed toxicity or progressive disease switch to a non-prespecified therapeutic or palliative strategy. This modification involved consideration of bivariate per-course outcomes encoding both efficacy and toxicity. We used numerical scores elicited from the trial's Principal Investigator to quantify the clinical desirability of each bivariate per-course outcome, and defined one endpoint as their average over all courses of treatment. Two other simpler sets of scores as well as log survival time also were used as endpoints. Estimation of each DTR-specific mean score was conducted using inverse probability weighted methods that assumed that missingness in the twelve remaining drop-outs was informative but explainable in that it only depended on past recorded data. We conducted additional worst-best case analyses to evaluate sensitivity of our findings to extreme departures from the explainable drop-out assumption.
我们对一项旨在比较晚期前列腺癌两阶段动态治疗方案(DTR)的临床试验数据进行了新的统计分析。试验方案规定,患者最初要在四种化疗方案中随机分组,对反应不佳的患者要重新随机分配到其余候选治疗方案之一。主要目的是比较DTR的总体成功率,成功的定义是患者连续两个疗程的治疗中均出现成功反应。在150名研究参与者中,有47人未按方案完成治疗。然而,其中35人未完成治疗的原因是无法进一步进行化疗,即出现毒性反应和/或疾病进展。因此,我们没有比较在这些患者继续接受指定化疗这种不切实际情况下DTR的总体成功率,而是进行了一项分析,比较了根据方案规定定义的可行转换规则,但增加了一项规定,即出现毒性反应或疾病进展的患者转换为未预先指定的治疗或姑息治疗策略。这种修改涉及考虑编码疗效和毒性的双变量每个疗程结局。我们使用从试验主要研究者那里得到的数值评分来量化每个双变量每个疗程结局的临床可取性,并将一个终点定义为所有治疗疗程的平均值。另外两组更简单的评分以及对数生存时间也用作终点。使用逆概率加权方法对每个DTR特定的平均评分进行估计,该方法假定其余12名退出者的数据缺失是有信息价值的,但可以解释,因为它仅取决于过去记录的数据。我们进行了额外的最坏-最好情况分析,以评估我们的研究结果对偏离可解释退出假设的极端情况的敏感性。