Parry Selina M, Berney Sue, Koopman René, Bryant Adam, El-Ansary Doa, Puthucheary Zudin, Hart Nicholas, Warrillow Stephen, Denehy Linda
Department of Physiotherapy, School of Health Sciences, The University of Melbourne, Melbourne, Australia.
BMJ Open. 2012 Sep 13;2(5). doi: 10.1136/bmjopen-2012-001891. Print 2012.
Intensive care-acquired weakness is a common problem, leads to significant impairment in physical functioning and muscle strength, and is prevalent in individuals with sepsis. Early rehabilitation has been shown to be safe and feasible; however, commencement is often delayed due to a patient's inability to co-operate. An intervention that begins early in an intensive care unit (ICU) admission without the need for patient volition may be beneficial in attenuating muscle wasting. The eRiCC (early rehabilitation in critical care) trial will investigate the effectiveness of functional electrical stimulation-assisted cycling and cycling alone, compared to standard care, in individuals with sepsis.
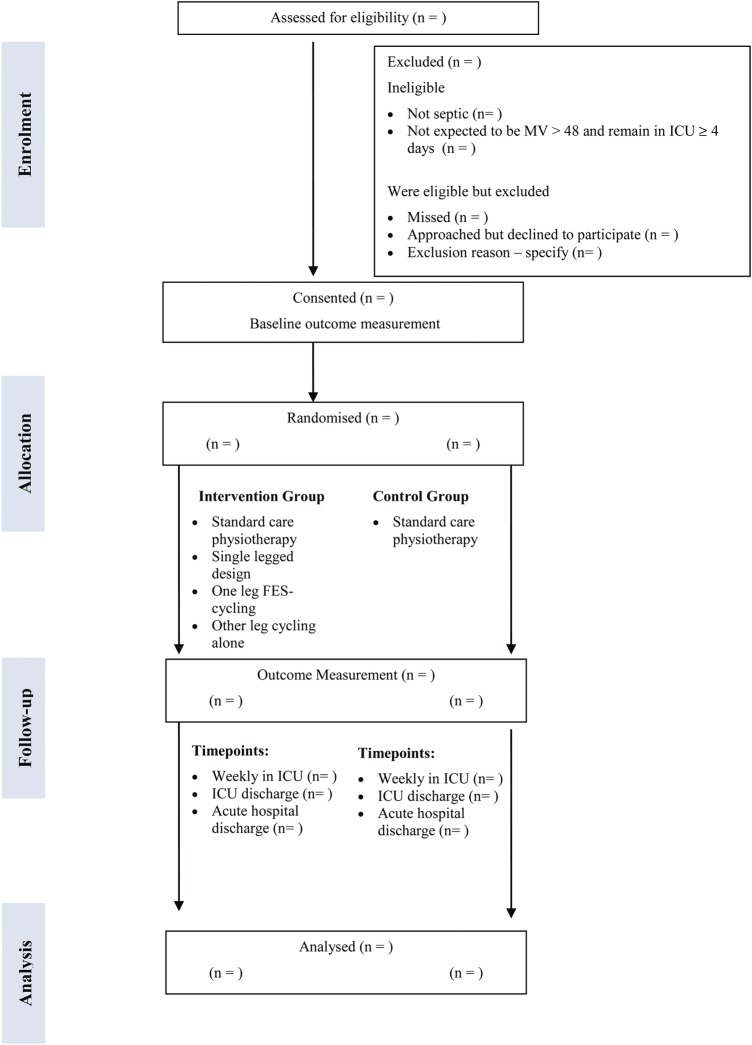
This is a single centre randomised controlled trial. Participants (n=80) aged ≥18 years, with a diagnosis of sepsis or severe sepsis, who are expected to be mechanically ventilated for ≥48 h and remain in the intensive care ≥4 days will be randomised within 72 h of admission to (1) standard care or (2) intervention where participants will receive functional electrical muscle stimulation-assisted supine cycling on one leg while the other leg undergoes cycling alone. Primary outcome measures include: muscle mass (quadriceps ultrasonography; bioelectrical impedance spectroscopy); muscle strength (Medical Research Council Scale; hand-held dynamometry) and physical function (Physical Function in Intensive Care Test; Functional Status Score in intensive care; 6 min walk test). Blinded outcome assessors will assess measures at baseline, weekly, at ICU discharge and acute hospital discharge. Secondary measures will be evaluated in a nested subgroup (n=20) and will consist of biochemical/histological analyses of collected muscle, urine and blood samples at baseline and at ICU discharge.
Ethics approval has been obtained from the relevant institution, and results will be published to inform clinical practice in the care of patients with sepsis to optimise rehabilitation and physical function outcomes.
Australian and New Zealand Clinical Trials Registry ACTRN12612000528853.
重症监护获得性肌无力是一个常见问题,会导致身体功能和肌肉力量严重受损,在脓毒症患者中很普遍。早期康复已被证明是安全可行的;然而,由于患者无法配合,康复往往会延迟开始。在重症监护病房(ICU)入院早期开始的、无需患者自主意愿的干预措施,可能有助于减轻肌肉萎缩。eRiCC(重症监护早期康复)试验将研究功能性电刺激辅助骑行和单纯骑行与标准护理相比,对脓毒症患者的有效性。
这是一项单中心随机对照试验。年龄≥18岁、诊断为脓毒症或严重脓毒症、预计机械通气≥48小时且在重症监护室停留≥4天的参与者(n = 80)将在入院72小时内随机分为(1)标准护理组或(2)干预组,干预组参与者将接受单腿功能性电肌肉刺激辅助仰卧骑行,而另一条腿进行单纯骑行。主要结局指标包括:肌肉质量(股四头肌超声检查;生物电阻抗光谱法);肌肉力量(医学研究委员会量表;手持测力计)和身体功能(重症监护物理功能测试;重症监护功能状态评分;6分钟步行试验)。盲法结局评估者将在基线、每周、ICU出院时和急性医院出院时评估各项指标。次要指标将在一个嵌套亚组(n = 20)中进行评估,包括在基线和ICU出院时对采集的肌肉、尿液和血液样本进行生化/组织学分析。
已获得相关机构的伦理批准,研究结果将发表,以为脓毒症患者的护理提供临床实践参考,以优化康复和身体功能结局。
澳大利亚和新西兰临床试验注册中心ACTRN12612000528853。