Center for Global Health, International Emergency and Refugee Health Branch, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
PLoS One. 2012;7(9):e44948. doi: 10.1371/journal.pone.0044948. Epub 2012 Sep 12.
International humanitarian aid workers providing care in emergencies are subjected to numerous chronic and traumatic stressors.
To examine consequences of such experiences on aid workers' mental health and how the impact is influenced by moderating variables.
We conducted a longitudinal study in a sample of international non-governmental organizations. Study outcomes included anxiety, depression, burnout, and life and job satisfaction. We performed bivariate regression analyses at three time points. We fitted generalized estimating equation multivariable regression models for the longitudinal analyses.
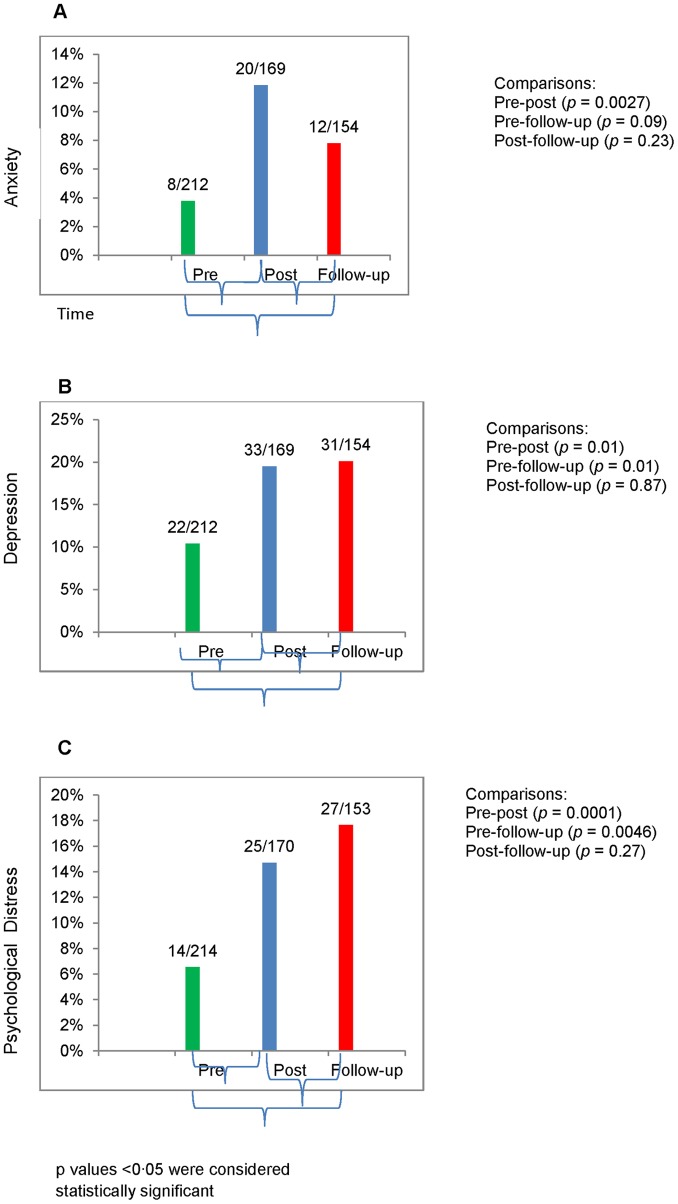
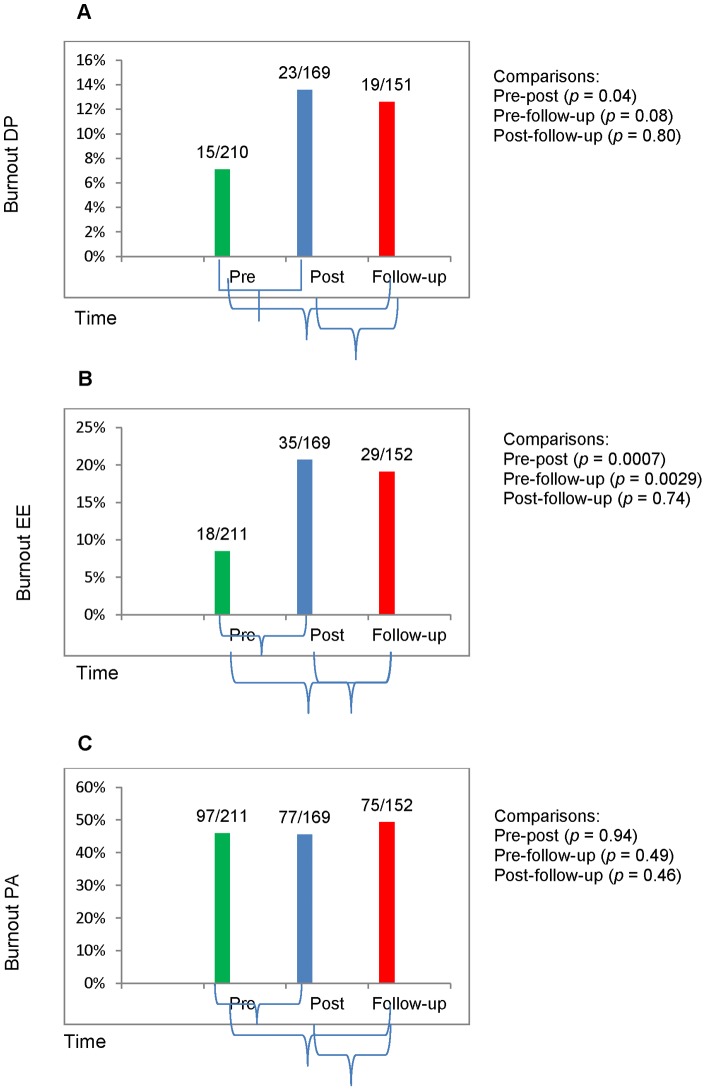
Study participants from 19 NGOs were assessed at three time points: 212 participated at pre-deployment; 169 (80%) post-deployment; and 154 (73%) within 3-6 months after deployment. Prior to deployment, 12 (3.8%) participants reported anxiety symptoms, compared to 20 (11.8%) at post-deployment (p = 0.0027); 22 (10.4%) reported depression symptoms, compared to 33 (19.5%) at post-deployment (p = 0.0117) and 31 (20.1%) at follow-up (p = .00083). History of mental illness (adjusted odds ratio [AOR] 4.2; 95% confidence interval [CI] 1.45-12.50) contributed to an increased risk for anxiety. The experience of extraordinary stress was a contributor to increased risk for burnout depersonalization (AOR 1.5; 95% CI 1.17-1.83). Higher levels of chronic stress exposure during deployment were contributors to an increased risk for depression (AOR 1.1; 95% CI 1.02-1.20) comparing post- versus pre-deployment, and increased risk for burnout emotional exhaustion (AOR 1.1; 95% CI 1.04-1.19). Social support was associated with lower levels of depression (AOR 0.9; 95% CI 0.84-0.95), psychological distress (AOR = 0.9; [CI] 0.85-0.97), burnout lack of personal accomplishment (AOR 0.95; 95% CI 0.91-0.98), and greater life satisfaction (p = 0.0213).
When recruiting and preparing aid workers for deployment, organizations should consider history of mental illness and take steps to decrease chronic stressors, and strengthen social support networks.
在紧急情况下提供护理的国际人道主义援助工作者面临着许多慢性和创伤性压力源。
研究这些经历对援助工作者心理健康的影响,以及调节变量如何影响这种影响。
我们对来自 19 个非政府组织的国际援助人员进行了一项纵向研究。研究结果包括焦虑、抑郁、倦怠、生活和工作满意度。我们在三个时间点进行了双变量回归分析。我们为纵向分析拟合了广义估计方程多变量回归模型。
来自 19 个非政府组织的研究参与者在三个时间点进行了评估:212 名参与者在部署前参加了评估;169 名(80%)参与者在部署后参加了评估;154 名(73%)参与者在部署后 3-6 个月内参加了评估。在部署前,有 12 名(3.8%)参与者报告有焦虑症状,而在部署后有 20 名(11.8%)参与者报告有焦虑症状(p = 0.0027);22 名(10.4%)参与者报告有抑郁症状,而在部署后有 33 名(19.5%)参与者报告有抑郁症状(p = 0.0117),有 31 名(20.1%)参与者在随访时有抑郁症状(p =.00083)。精神病史(调整后的优势比[OR]4.2;95%置信区间[CI]1.45-12.50)增加了焦虑的风险。经历特殊压力是导致倦怠去人性化(调整后的 OR 1.5;95%CI 1.17-1.83)风险增加的原因。在部署期间经历更高水平的慢性压力暴露会增加抑郁(调整后的 OR 1.1;95%CI 1.02-1.20)的风险,与部署前相比,并且会增加倦怠情绪耗竭(调整后的 OR 1.1;95%CI 1.04-1.19)的风险。社会支持与较低水平的抑郁(调整后的 OR 0.9;95%CI 0.84-0.95)、心理困扰(调整后的 OR = 0.9;[CI]0.85-0.97)、倦怠缺乏个人成就感(调整后的 OR 0.95;95%CI 0.91-0.98)和更高的生活满意度(p = 0.0213)相关。
在招募和为援助人员部署做准备时,组织应考虑精神病史,并采取措施减少慢性压力源,加强社会支持网络。